
Abstract
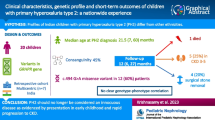
The rarity of primary hyperoxaluria (PH) challenges our understanding of the disease. The purpose of our study was to describe the course of clinical care in a United States cohort of PH pediatric patients, highlighting health service utilization. We performed a retrospective cohort study of PH patients < 18 years old in the PEDSnet clinical research network from 2009 to 2021. Outcomes queried included diagnostic imaging and testing related to known organ involvement of PH, surgical and medical interventions specific to PH-related renal disease, and select PH-related hospital service utilization. Outcomes were evaluated relative to cohort entrance date (CED), defined as date of first PH-related diagnostic code. Thirty-three patients were identified: 23 with PH type 1; 4 with PH type 2; 6 with PH type 3. Median age at CED was 5.0 years (IQR 1.4, 9.3 years) with the majority being non-Hispanic white (73%) males (70%). Median follow-up between CED and most recent encounter was 5.1 years (IQR 1.2, 6.8). Nephrology and Urology were the most common specialties involved in care, with low utilization of other sub-specialties (12%-36%). Most patients (82%) had diagnostic imaging used to evaluate kidney stones; 11 (33%) had studies of extra-renal involvement. Stone surgery was performed in 15 (46%) patients. Four patients (12%) required dialysis, begun in all prior to CED; four patients required renal or renal/liver transplant.
Conclusion: In this large cohort of U.S. PH children, patients required heavy health care utilization with room for improvement in involving multi-disciplinary specialists.
What is Known: • Primary hyperoxaluria (PH) is rare with significant implications on patient health. Typical involvement includes the kidneys; however, extra-renal manifestations occur. • Most large population studies describe clinical manifestations and involve registries. | |
What is New: • We report the clinical journey, particularly related to diagnostic studies, interventions, multispecialty involvement, and hospital utilization, of a large cohort of PH pediatric patients in the PEDSnet clinical research network. • There are missed opportunities, particularly in that of specialty care, that could help in the diagnosis, treatment, and even prevention of known clinical manifestations. |
Similar content being viewed by others

Abbreviations
- CED:
-
Cohort entrance date
- CDM:
-
Common data model
- CKD:
-
Chronic kidney disease
- ED:
-
Emergency Department
- EHR:
-
Electronic health records
- ESRD:
-
End stage renal disease
- ESWL:
-
Extracorporeal shockwave lithotripsy
- OMOP:
-
Observational Medical Outcomes Partnership
- PCNL:
-
Percutaneous nephrolithotomy
- PH:
-
Primary hyperoxaluria
- URS:
-
Ureteroscopy
References
Hopp K, Cogal AG, Bergstralh EJ, Seide BM, Olson JB, Meek AM et al (2015) Phenotype-Genotype Correlations and Estimated Carrier Frequencies of Primary Hyperoxaluria. J Am Soc Nephrol 26:2559–2570. https://doi.org/10.1681/ASN.2014070698
Hoppe B, Beck BB, Milliner DS (2009) The primary hyperoxalurias. Kidney Int 75:1264–1271. https://doi.org/10.1038/ki.2009.32
Ventzke A, Feldkotter M, Wei A, Becker J, Beck BB, Hoppe B (2017) Systematic assessment of urinary hydroxy-oxo-glutarate for diagnosis and follow-up of primary hyperoxaluria type III. Pediatr Nephrol 32:2263–71. https://doi.org/10.1007/s00467-017-3731-3
Lieske JC, Monico CG, Holmes WS, Bergstralh EJ, Slezak JM, Rohlinger AL et al (2005) International registry for primary hyperoxaluria. Am J Nephrol 25:290–6. https://doi.org/10.1159/000086360
van der Hoeven SM, van Woerden CS, Groothoff JW (2012) Primary hyperoxaluria type 1, a too often missed diagnosis and potentially treatable cause of end-stage renal disease in adults: results of the Dutch cohort. Nephrol Dial Transplant 27:3855–3862. https://doi.org/10.1093/ndt/gfs320
Kamoun A, Lakhoua R (1996) End-stage renal disease of the Tunisian child: epidemiology, etiologies, and outcome. Pediatr Nephrol 10:479–482. https://doi.org/10.1007/s004670050143
Harambat J, van Stralen KJ, Espinosa L, Groothoff JW, Hulton SA, Cerkauskiene R et al (2012) Characteristics and outcomes of children with primary oxalosis requiring renal replacement therapy. Clin J Am Soc Nephrol 7:458–465. https://doi.org/10.2215/CJN.07430711
Lefaki I, Papageorgiou M, Karteridou A, Dotis J, Koteli C, Printza N et al (2014) Secondary perforating dermatosis in an infant with primary hyperoxaluria type I. Eur J Dermatol 24:254–255. https://doi.org/10.1684/ejd.2014.2281
Soliman NA, Nabhan MM, Abdelrahman SM, Abdelaziz H, Helmy R, Ghanim K et al (2017) Clinical spectrum of primary hyperoxaluria type 1: Experience of a tertiary center. Nephrol Ther 13:176–82. https://doi.org/10.1016/j.nephro.2016.08.002
Fishbein GA, Micheletti RG, Currier JS, Singer E, Fishbein MC (2008) Atherosclerotic oxalosis in coronary arteries. Cardiovasc Pathol 17:117–123. https://doi.org/10.1016/j.carpath.2007.07.002
Rao NM, Yallapragada A, Winden KD, Saver J, Liebeskind DS (2014) Stroke in primary hyperoxaluria type I. J Neuroimaging 24:411–3. https://doi.org/10.1111/jon.12020
Dierselhuis EF, Maathuis PG (2013) Conservative treatment of a pathological fracture in a 3-year-old boy with primary hyperoxaluria type I. J Pediatr Orthop B 22:175–7. https://doi.org/10.1097/BPB.0b013e32834fe880
Sangave AA, Gearinger MD, Diloreto DA (2017) Crystalline Retinopathy from Hyperoxaluria: Long-Term Follow-Up. Retin Cases Brief Rep 11:1–3. https://doi.org/10.1097/ICB.0000000000000272
Forrest CB, Margolis PA, Bailey LC, Marsolo K, Del Beccaro MA, Finkelstein JA et al (2014) PEDSnet: a National Pediatric Learning Health System. J Am Med Inform Assoc 21:602–6. https://doi.org/10.1136/amiajnl-2014-002743
Kuhlthau KA, Bailey LC, Baer BL, Coury DL, Law JK, Murray DS et al (2018) Large Databases for Pediatric Research on Children with Autism Spectrum Disorder. J Dev Behav Pediatr 39:168–76. https://doi.org/10.1097/DBP.0000000000000534
Hubbard RA, Huang J, Harton J, Oganisian A, Choi G, Utidjian L et al (2019) A Bayesian latent class approach for EHR-based phenotyping. Stat Med 38:74–87. https://doi.org/10.1002/sim.7953
Phillips CA, Razzaghi H, Aglio T, McNeil MJ, Salvesen-Quinn M, Sopfe J et al (2019) Development and evaluation of a computable phenotype to identify pediatric patients with leukemia and lymphoma treated with chemotherapy using electronic health record data. Pediatr Blood Cancer 66:e27876. https://doi.org/10.1002/pbc.27876
Denburg MR, Razzaghi H, Bailey LC, Soranno DE, Pollack AH, Dharnidharka VR et al (2019) Using Electronic Health Record Data to Rapidly Identify Children with Glomerular Disease for Clinical Research. J Am Soc Nephrol 30:2427–2435. https://doi.org/10.1681/ASN.2019040365
Khare R, Kappelman MD, Samson C, Pyrzanowski J, Darwar RA, Forrest CB et al (2020) Development and evaluation of an EHR-based computable phenotype for identification of pediatric Crohn's disease patients in a National Pediatric Learning Health System. Learn Health Syst 4:e10243. https://doi.org/10.1002/lrh2.10243
Tasian G, Dickinson K, Karafilidis J, Marchesani N, Antunes N, Razzaghi H et al (2022) Diagnostic Code-Based Screening for Identifying Children with Primary Hyperoxaluria. J Urol 208(4):898–905. https://doi.org/10.1097/JU.0000000000002863
Office of the National Coordinator for Health Information Technology DoH, Human S (2012) Health information technology: standards, implementation specifications, and certification criteria for electronic health record technology, 2014 edition; revisions to the permanent certification program for health information technology. Final rule. Fed Regist 77:54163–292
Mucha L, Hoppe B, Silber A, Wang Z, Miyasato G, Skaar JR et al (2022) Clinical and economic impact of primary hyperoxaluria: a retrospective claims analysis. J Manag Care Spec Pharm 28:316–23. https://doi.org/10.18553/jmcp.2022.28.3.316
Mandrile G, Pelle A, Sciannameo V, Benetti E, D’Alessandro MM, Emma F et al (2022) Primary hyperoxaluria in Italy: the past 30 years and the near future of a (not so) rare disease. J Nephrol 35:841–850. https://doi.org/10.1007/s40620-022-01258-4
Talati JJ, Hulton SA, Garrelfs SF, Aziz W, Rao S, Memon A et al (2018) Primary hyperoxaluria in populations of Pakistan origin: results from a literature review and two major registries. Urolithiasis 46:187–195. https://doi.org/10.1007/s00240-017-0996-8
Gargah T, Khelil N, Youssef G, Karoui W, Lakhoua MR, Abdelmoula J (2012) Primary hyperoxaluria type 1 in Tunisian children. Saudi J Kidney Dis Transpl 23:385–390
Jellouli M, Ferjani M, Abidi K, Zarrouk C, Naija O, Abdelmoula J et al (2016) Primary hyperoxaluria in infants. Saudi J Kidney Dis Transpl 27:526–532. https://doi.org/10.4103/1319-2442.182389
Solmos GR, Ali A, Rodby RA, Fordham EW (1994) Rapid reversal of bone scan abnormalities in a patient with type 1 primary hyperoxaluria and oxalosis. Clin Nucl Med 19:769–772. https://doi.org/10.1097/00003072-199409000-00004
Kemper MJ, Muller-Wiefel DE (1996) Nephrocalcinosis in a patient with primary hyperoxaluria type 2. Pediatr Nephrol 10:442–444. https://doi.org/10.1007/s004670050135
Alsuwaida A, Hayat A, Alwakeel JS (2007) Oxalosis presenting as early renal allograft failure. Saudi J Kidney Dis Transpl 18:253–256
Orazi C, Picca S, Schingo PM, Fassari FM, Canepa G (2009) Oxalosis in primary hyperoxaluria in infancy : Report of a case in a 3-month-old baby. Follow-up for 3 years and review of literature. Skeletal Radiol 38:387–391. https://doi.org/10.1007/s00256-008-0625-2
Khan Z, Sciveres M, Salis P, Minervini M, Maggiore G, Cintorino D et al (2011) Combined split liver and kidney transplantation in a three-year-old child with primary hyperoxaluria type 1 and complete thrombosis of the inferior vena cava. Pediatr Transplant 15:E64-70. https://doi.org/10.1111/j.1399-3046.2009.01241.x
Dieudonne Y, Eprinchard L, Leon E, Oswald P, Gressel A, Carre S et al (2018) Paraplegia as a presentation of primary hyperoxaluria. CEN Case Rep 7:313–315. https://doi.org/10.1007/s13730-018-0349-7
Al Riyami MS, Al Ghaithi B, Al Hashmi N, Al Kalbani N (2015) Primary hyperoxaluria type 1 in 18 children: genotyping and outcome. Int J Nephrol 2015:634175. https://doi.org/10.1155/2015/634175
Gargah T, Khelil N, Gharbi Y, Karoui W, Trabelsi M, Rajhi H et al (2011) Primary hyperoxaluria type 1 in Tunisian children. Tunis Med 89:163–167
Almardini RI, Alfarah MG, Salaita GM (2014) The clinical pattern of primary hyperoxaluria in pediatric patient at Queen Rania Abdulla Children Hospital. Arab J Nephrol Transplant 7:119–123
Rhuma NR, Fituri OA, Sabei LT (2018) Mutational analysis of AGXT gene in Libyan children with primary hyperoxaluria type 1 at Tripoli Children Hospital. Saudi J Kidney Dis Transpl 29:30–38. https://doi.org/10.4103/1319-2442.225202
Fadel FI, Kotb MA, Abdel Mawla MA, Hasanin RM, Salem AM, Fathallah MG et al (2022) Primary hyperoxaluria type 1 in children: Clinical classification, renal replacement therapy, and outcome in a single centre experience. Ther Apher Dial 26:162–170. https://doi.org/10.1111/1744-9987.13666
Sas DJ, Enders FT, Mehta RA, Tang X, Zhao F, Seide BM et al (2020) Clinical features of genetically confirmed patients with primary hyperoxaluria identified by clinical indication versus familial screening. Kidney Int 97:786–792. https://doi.org/10.1016/j.kint.2019.11.023
Singh P, Viehman JK, Mehta RA, Cogal AG, Hasadsri L, Oglesbee D et al (2022) Clinical characterization of primary hyperoxaluria type 3 in comparison with types 1 and 2. Nephrol Dial Transplant 37:869–875. https://doi.org/10.1093/ndt/gfab027
Garrelfs SF, Rumsby G, Peters-Sengers H, Erger F, Groothoff JW, Beck BB et al (2019) Patients with primary hyperoxaluria type 2 have significant morbidity and require careful follow-up. Kidney Int 96:1389–1399. https://doi.org/10.1016/j.kint.2019.08.018
Martin-Higueras C, Garrelfs SF, Groothoff JW, Jacob DE, Moochhala SH, Bacchetta J et al (2021) A report from the European Hyperoxaluria Consortium (OxalEurope) Registry on a large cohort of patients with primary hyperoxaluria type 3. Kidney Int 100:621–635. https://doi.org/10.1016/j.kint.2021.03.031
Strauss SB, Waltuch T, Bivin W, Kaskel F, Levin TL (2017) Primary hyperoxaluria: spectrum of clinical and imaging findings. Pediatr Radiol 47:96–103. https://doi.org/10.1007/s00247-016-3723-7
Hoppe B, Langman CB (2003) A United States survey on diagnosis, treatment, and outcome of primary hyperoxaluria. Pediatr Nephrol 18:986–991. https://doi.org/10.1007/s00467-003-1234-x
Cochat P, Hulton SA, Acquaviva C, Danpure CJ, Daudon M, De Marchi M et al (2012) Primary hyperoxaluria Type 1: indications for screening and guidance for diagnosis and treatment. Nephrol Dial Transplant 27:1729–36. https://doi.org/10.1093/ndt/gfs078
Garrelfs SF, Frishberg Y, Hulton SA, Koren MJ, O’Riordan WD, Cochat P et al (2021) Lumasiran, an RNAi Therapeutic for Primary Hyperoxaluria Type 1. N Engl J Med 384:1216–1226. https://doi.org/10.1056/NEJMoa2021712
Forbes TA, Brown BD, Lai C (2022) Therapeutic RNA interference: A novel approach to the treatment of primary hyperoxaluria. Br J Clin Pharmacol 88:2525–2538. https://doi.org/10.1111/bcp.14925
Meaux MN, Sellier-Leclerc AL, Acquaviva-Bourdain C, Harambat J, Allard L, Bacchetta J (2022) The effect of lumasiran therapy for primary hyperoxaluria type 1 in small infants. Pediatr Nephrol 37:907–11. https://doi.org/10.1007/s00467-021-05393-1
Hayes W, Sas DJ, Magen D, Shasha-Lavsky H, Michael M, Sellier-Leclerc AL et al (2022) Efficacy and safety of lumasiran for infants and young children with primary hyperoxaluria type 1: 12-month analysis of the phase 3 ILLUMINATE-B trial. Pediatr Nephrol online ahead of print. https://doi.org/10.1007/s00467-022-05684-1
Lagies R, Udink Ten Cate FEA, Feldkotter M, Beck BB, Sreeram N, Hoppe B et al (2019) Subclinical myocardial disease in patients with primary hyperoxaluria and preserved left ventricular ejection fraction: a two-dimensional speckle-tracking imaging study. Pediatr Nephrol 34:2591–2600. https://doi.org/10.1007/s00467-019-04330-7
Beck BB, Hoppe B (2006) Is there a genotype-phenotype correlation in primary hyperoxaluria type 1? Kidney Int 70:984–986. https://doi.org/10.1038/sj.ki.5001797
Acknowledgements
Elements of this study was made possible through funding by Dicerna Pharmaceuticals.
Funding
This work was supported by Dicerna Pharmaceuticals.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design (Christina B. Ching, Kimberley Dickinson, John Karafilidis, Nicole Marchesani, Lisa Mucha, Nuno Antunes, Hanieh Razzaghi, Levon Utidjian, Karyn Yonekawa, Douglas E. Coplen, Samina Muneeruddin, Bob DeFoor, Kyle Rove, Christopher B. Forrest, Gregory E. Tasian). Material preparation, data collection and analysis were performed by (Christina B. Ching, Kimberley Dickinson, Gregory E. Tasian). The first draft of the manuscript was written by Christina B. Ching and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
This study was performed in line with principles of the Declaration of Helsinki. Approval was granted by the Children’s Hospital of Philadelphia Institutional Review Board under the PEDSnet Master Protocol (IRB# 16-012878).
Competing interests
Gregory Tasian is on the Scientific Advisory Board for Dicerna Pharmaceuticals, a Novo Nordisk Company, and Alnylam Pharmaceuticals.
Additional information
Communicated by Gregorio Milani
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ching, C.B., Dickinson, K., Karafilidis, J. et al. The real world experience of pediatric primary hyperoxaluria patients in the PEDSnet clinical research network. Eur J Pediatr 182, 4027–4036 (2023). https://doi.org/10.1007/s00431-023-05077-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-023-05077-y