
Abstract
Purpose
This study compares the short- and long-term outcomes between the left thoraco-abdominal and trans-abdominal approaches for radical resection of adenocarcinoma of the gastro-esophageal junction (GEJ) (Siewert types II and III) following neo-adjuvant chemotherapy.
Methods
A retrospective analysis of a prospectively maintained database of patients from May 2008 to December 2016. Demographic variables, perioperative outcomes, and survival were compared between two approaches.
Results
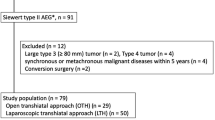
Of the 792 patients, who underwent total/proximal gastrectomy during the specified time interval, 162 had Siewert’s type II/III lesions, of which 147 received neoadjuvant chemotherapy and were included in the study. Ninety-two and 55 patients underwent definitive surgery through trans-abdominal and left thoraco-abdominal approach respectively. On baseline endoscopy, 81.8% of patients in the left thoraco-abdominal group had lower esophageal mucosal infiltration as compared to 41.3% in the trans-abdominal group (p < 0.001). Both groups were comparable in terms of duration of surgery, blood loss, complications, severity of complications (Clavien-Dindo grade), duration of hospital stay, R0 resection rate, length of proximal margin, and lymph node yield. At a median follow-up of 24 months, there was no difference in recurrence rate and survival between the groups.
Conclusion
Both left thoraco-abdominal and trans-abdominal are comparable surgical approaches for tumors involving the GEJ in terms of morbidity, perioperative, and long-term oncological outcomes. In patients with lower esophageal involvement, the left thoraco-abdominal approach is a feasible alternative with no added overall morbidity or mortality and can be preferred especially in cases, where a safe proximal margin and anastomosis is deemed technically challenging.



Similar content being viewed by others


Data availability
Will be provided on request.
References
Lin D, Khan U, Goetze TO et al (2019) Gastroesophageal junction adenocarcinoma: is there an optimal management? Am Soc Clin Oncol Educ Book 39:e88–e95
Siewert JR, Stein HJ (1996) Adenocarcinoma of the gastroesophageal junction: classification, pathology and extent of resection. Dis Esophagus 9:173–182
Kurokawa Y, Sasako M, Doki Y (2013) Treatment approaches to esophagogastric junction tumors. Dig Surg 30(2):169–173
DeMeester SR (2006) Adenocarcinoma of the esophagus and cardia: a review of the disease and its treatment. Ann Surg Oncol 13:12–30
Mariette C, Piessen G, Briez N, Gronnier C, Triboulet JP (2011) Oesophagogastric junction adenocarcinoma: which therapeutic approach? Lancet Oncol 12:296–305
Ferro A, Peleteiro B, Malvezzi M, Bosetti C, Bertuccio P, Levi F, Negri E, la Vecchia C, Lunet N (2014) Worldwide trends in gastric cancer mortality (1980-2011), with predictions to 2015, and incidence by subtype. Eur J Cancer 50:1330–1344
Kurokawa Y, Sasako M, Sano T et al (2015) Japan Clinical Oncology Group (JCOG9502). Ten-year follow up results of a randomized clinical trial comparing left thoracoabdominal and abdominal transhiatal approaches to total gastrectomy for adenocarcinoma of the oesophagogastric junction or gastric cardia. Br J Surg 102(4):341–348
Sasako M, Sano T, Yamamoto S, Sairenji M, Arai K, Kinoshita T, Nashimoto A, Hiratsuka M (2006) Left thoracoabdominal approach versus abdominal – transhiatal approach for gastric cancer of the cardia or sub cardia: a randomized controlled trial. Lancet Oncol 7:644–651
Sobin LH, Gospodarowicz M, Wittekind C (2009) TNM classification of malignant tumours. 7th. UICC International Union Against Cancer. New York: Wiley-Blackwell
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Kauppila JH, Lagergren J (2016) The surgical management of esophago-gastric junctional cancer. Surg Oncol 25(4):394–400
Hashimoto T, Kurokawa Y, Mori M, Doki Y (2018) Surgical treatment of gastroesophageal junction cancer. J Gastric Cancer 18(3):209–217
Amin MB, Edge SB, Greene FL (2017) AJCC cancer staging manual (ed 8). Springer, New York
Hulscher JB, van Sandick JW, de Boer AG et al (2002) Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med 347:1662–1669
National Comprehensive Cancer Network. Esophageal and esophagogastric junction cancers (Version 1.2020). https://www.nccn.org/professionals/physician_gls/pdf/esophageal.pdf. Accessed Apr 7, 2020
Al-Batran SE, Lorenzen S (2017) Management of locally advanced gastroesophageal cancer: still a multidisciplinary global challenge? Hematol Oncol Clin North Am 31:441–452
Coccolini F, Nardi M, Montori G, Ceresoli M, Celotti A, Cascinu S, Fugazzola P, Tomasoni M, Glehen O, Catena F, Yonemura Y, Ansaloni L (2018) Neoadjuvant chemotherapy in advanced gastric and esophago-gastric cancer. Meta-analysis of randomized trials. Int J Surg 51:120–127
Ychou M, Boige V, Pignon J-P, Conroy T, Bouché O, Lebreton G, Ducourtieux M, Bedenne L, Fabre JM, Saint-Aubert B, Genève J, Lasser P, Rougier P (2011) Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol 29:1715–1721
Cunningham D, Allum WH, Stenning SP, Thompson JN, van de Velde CJH, Nicolson M, Scarffe JH, Lofts FJ, Falk SJ, Iveson TJ, Smith DB, Langley RE, Verma M, Weeden S, Chua YJ (2006) Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 355:11–20
Sirohi B, Barreto SG, Singh A, Batra S, Mittra A, Rastogia S, Ramadwar M, Shetty N, Goel M, Shrikhande SV (2014) Epirubicin, oxaliplatin, and capecitabine is just as “MAGIC”al as epirubicin, cisplatin, and fluorouracil perioperative chemotherapy for resectable locally advanced gastro-oesophageal cancer. J Cancer Res Ther 10:866–870
Alderson D, Cunningham D, Nankivell M, Blazeby JM, Griffin SM, Crellin A, Grabsch HI, Langer R, Pritchard S, Okines A, Krysztopik R, Coxon F, Thompson J, Falk S, Robb C, Stenning S, Langley RE (2017) Neoadjuvant cisplatin and fluorouracil versus epirubicin, cisplatin, and capecitabine followed by resection in patients with oesophageal adenocarcinoma (UK MRC OE05): an open-label, randomised phase 3 trial. Lancet Oncol 18(9):1249–1260
Al-Batran S-E, Homann N, Pauligk C et al (2019) Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet 393(10184):1948–1957
Grotenhuis BA, Wijnhoven BP, van Marion R et al (2009) The sentinel node concept in adenocarcinomas of the distal esophagus and gastroesophageal junction. J Thorac Cardiovasc Surg 138:608–612
Rüdiger Siewert J, Feith M, Werner M et al (2000) Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg 232:353–361
Kurokawa Y, Hiki N, Yoshikawa T, Kishi K, Ito Y, Ohi M, Wada N, Takiguchi S, Mine S, Hasegawa S, Matsuda T, Takeuchi H (2015) Mediastinal lymph node metastasis and recurrence in adenocarcinoma of the esophagogastric junction. Surgery 157:551–555
Nunobe S, Ohyama S, Sonoo H, Hiki N, Fukunaga T, Seto Y, Yamaguchi T (2008) Benefit of mediastinal and para-aortic lymph-node dissection for advanced gastric cancer with esophageal invasion. J Surg Oncol 97:392–395
Nakamura M, Iwahashi M, Nakamori M, Naka T, Ojima T, Iida T, Katsuda M, Tsuji T, Hayata K, Mastumura S, Yamaue H (2012) Lower mediastinal lymph node metastasis is an independent survival factor of Siewert type II and III adenocarcinomas in the gastroesophageal junction. Am Surg 78(5):567–573
Han WH, Eom BW, Yoon HM, Reim D, Kim YW, Kim MS, Lee JM, Ryu KW (2019) The optimal extent of lymph node dissection in gastroesophageal junctional cancer: retrospective case control study. BMC Cancer 19(1):719. https://doi.org/10.1186/s12885-019-5922-8
Kurokawa Y, Sasako M, Sano T, Shibata T, Ito S, Nashimoto A, Kurita A, Kinoshita T, for the Japan Clinical Oncology Group (2011) Functional outcomes after extended surgery for gastric cancer. Br J Surg 98:239–245
Author information
Authors and Affiliations
Contributions
NK, AD, MB, VC, and SS participated in study conception and design. NK, JM, and GK participated in acquisition of data. NK, AD, MB, VO, VC, and SS participated in analysis and interpretation of data. NK, AD, MB, JM, GK VO, VC, and SS participated in drafting of manuscript. NK, AD, MB, VC, VO, and SS participated in critical revision of manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
This research study was conducted retrospectively from data obtained for clinical purposes. No institutional research committee approval was required as this was a retrospective study.
Consent to participate
Written informed consent was obtained from the patient.
Consent for publication
Written informed consent for publication of their clinical details was obtained from the patient.
Code availability
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kumar, N.A., Desouza, A., Bhandare, M.S. et al. Curative resection for adenocarcinoma of the gastro-esophageal junction following neo-adjuvant chemotherapy—thoraco-abdominal vs. trans-abdominal approach. Langenbecks Arch Surg 406, 613–621 (2021). https://doi.org/10.1007/s00423-020-02020-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-020-02020-9