
Abstract
Background
Large middle-third esophageal diverticula are rare. Thoracotomy has been proposed as mainstay of treatment; however, minimally invasive resection through lateral or prone position thoracoscopy has been described.
Methods
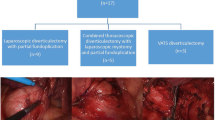
The technical aspects of the novel semi-prone minimally invasive thoracoscopy (spVATS) in the management of large (> 5 cm) infracarinal traction diverticula are described. Operative outcomes, pre- and postoperative symptoms (Eckardt score) and quality of life (Short-Form 36) are analyzed.
Results
Four symptomatic patients underwent spVATS for traction midesophageal diverticula. The median age was 59 years and 75% were males. The median diverticulum size was 7.0 cm (range 5.5–8). The median preoperative Eckardt score was 8.4 (range 5–10), and the overall incidence of respiratory symptoms was 50%. Esophageal manometry was performed in three patients with no evidence of underlying motility disorders. The median operative time was 149 min (range 125–175). No intraoperative complications or open conversions occurred. Postoperative morbidity and mortality were 25% and 0%, respectively. The median hospital length of stay was 7.5 days (range 6–10). The median postoperative follow-up was 22 months (range 5–35). At the last follow-up, there was a significant improvement of patients’ symptoms (p = 0.024) and quality of life (p < 0.05) with complete resolution of respiratory symptoms.
Conclusion
In summary, spVATS seems a valuable approach to treat large midesophageal traction diverticula in centers experienced with minimally invasive esophageal surgery. Further studies are needed to validate the advantages and promising outcomes of the spVATS providing more robust evidence on the treatment of this rare clinical entity.








Similar content being viewed by others


References
Kauffels A, Schuld J, Schilling MK, Kollmar O (2012) Giant midoesophageal diverticulum--case report and review of the literature. J Gastrointest Surg 16(6):1240–1244
Michael H, Fisher RS (2004) Treatment of epiphrenic and mid-esophageal diverticula. Curr Treat Options Gastroenterol 7(1):41–52
Chan DSY, Foliaki A, Lewis WG, Clark GWB, Blackshaw GRJC (2017) Systematic review and meta-analysis of surgical treatment of non-Zenker’s Oesophageal diverticula. J Gastrointest Surg 21(6):1067–1075
Macke RA, Luketich JD, Pennathur A, Bianco V, Awais O, Gooding WE, Christie NA, Schuchert MJ, Nason KS, Levy RM (2015) Thoracic esophageal diverticula: a 15-year experience of minimally invasive surgical management. Ann Thorac Surg 100(5):1795–1802
Caronia FP, Fiorelli A, Santini M, Lo Monte AI (2017) Uniportal video-assisted thoracoscopic surgery resection of a giant midesophageal diverticulum. Ann Thorac Surg 103(4):e365–e367
Chandeze MM, Gayet B, Cowan J, Ferraz JM, Fuks D (2019) Resection of an esophageal diverticulum by thoracoscopy in prone position. Ann Thorac Surg 107(2):e153–e155
Palanivelu C, Rangarajan M, Maheshkumaar GS, Senthilkumar R (2008) Minimally invasive surgery combined with peroperative endoscopy for symptomatic middle and lower esophageal diverticula: a single institute’s experience. Surg Laparosc Endosc Percutan Tech 18(2):133–138
Fernando HC, Luketich JD, Samphire J, Alvelo-Rivera M, Christie NA, Buenaventura PO, Landreneau RJ (2005) Minimally invasive operation for esophageal diverticula. Ann Thorac Surg 80(6):2076–2080
Bonavina L, Asti E, Sironi A, Bernardi D, Aiolfi A (2017) Hybrid and total minimally invasive esophagectomy: how I do it. J Thorac Dis 9(Suppl 8):S761–S772
Bonavina L, Aiolfi A, Siboni S, Rausa E (2014) Thoracoscopic removal of dental prosthesis impacted in the upper thoracic esophagus. World J Emerg Surg 9(1):5
Eckardt VF (2001) Clinical presentations and complications of achalasia. Gastrointest Endosc Clin N Am 11(2):281–292 vi
Apolone G, Mosconi P (1998) The Italian SF-36 health survey: translation, validation and norming. J Clin Epidemiol 51:1025–1036
Eckardt VF, Aignherr C, Bernhard G (1992) Predictors of outcome in patients with achalasia treated by pneumatic dilatation. Gastroenterol 103:1732–1738
Ford AC, Forman D, Moayyedi P, Morice AH (2006) Cough in the community: a cross sectional survey and the relationship to gastrointestinal symptoms. Thorax 61:975–979
Marik PE (2001) Aspiration pneumonitis and aspiration pneumonia. N Engl J Med 344(9):665–671
Bonavina L, Laface L, Abate E, Punturieri M, Agosteo M, Nencioni M (2012) Comparison of ventilation and cardiovascular parameters between prone thoracoscopic and Ivor Lewis esophagectomy. Updat Surg 64:81–85
Author information
Authors and Affiliations
Contributions
The manuscript was conceived and designed by Aiolfi, Micheletto, Jonghi-Lavarini, and Bona. The literature was acquired and reviewed by Aiolfi, Tringali, and Bonitta. The manuscript was drafted by Aiolfi and Bona and critically revised by Micheletto and Campanelli. Final approval for publication of this manuscript has been given by all authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards;
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Aiolfi, A., Micheletto, G., Tringali, D. et al. Semi-prone video-assisted thoracoscopy for the treatment of large infracarinal traction diverticula. Langenbecks Arch Surg 404, 771–777 (2019). https://doi.org/10.1007/s00423-019-01801-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-019-01801-1