
Abstract
Purpose
Respiratory complications are responsible to a high degree for postoperative morbidity and mortality after Ivor-Lewis esophagectomy. The etiology of respiratory failure is known to be multifactorial with preoperative impaired lung function being the most important one. The aim of this study was to investigate the correlation between preoperative airway colonization (PAC) and postoperative respiratory complications.
Methods
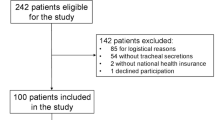
In this observational study, 64 patients with esophageal cancer were included. All patients underwent Ivor-Lewis esophagectomy with laparoscopic or open gastric mobilization. After induction of anesthesia and intubation with a double-lumen tube, bronchial exudate was collected by random endoluminal suction for further microbiological work-up. Length of postoperative mechanical ventilation (<24 h, 24–72 h, >72 h), re-intubation, and tracheostomy were recorded as primary and secondary study endpoints.
Results
In 13 of 64 study patients (20.3 %), pathological colonization of the bronchial airways could be proved prior to esophagectomy. Haemophilus species was the most frequently identified pathogen. PAC was associated with a longer history of smoking (p = 0.025), a lower preoperative forced expiratory volume (FEV1, p = 0.009) or vital capacity (VC, p = 0.038), a prolonged postoperative mechanical ventilation (p < 0.001), and a higher frequency of re-intubation (p < 0.001) and tracheostomy (p = 0.017). In the multivariate analysis, PAC was identified as an independent predictor of respiratory failure (hazard ratio 11.4, 95 % confidence interval 2.6–54, p = 0.002). Mortality in the PAC group was 30.8 % compared to 0 % in patients without PAC (p < 0.0001).
Conclusion
PAC is a significant risk factor for postoperative respiratory failure. A routine bronchoscopy and bronchoalveolar lavage as part of preoperative management prior to esophagectomy need to be discussed.
Similar content being viewed by others

References
Karl RC, Schreiber R, Boulware D, Baker S, Coppola D (2000) Factors affecting morbidity, and survival in patients undergoing Ivor Lewis esophagogastrectomy. Ann Surg 231:635–643
Hulscher JB, Tijssen JG, Obertop H, van Lanschot JJ (2001) Transthoracic versus transhiatal resection for carcinoma of the esophagus: a metaanalysis. Ann Thorac Surg 72:306–313
Ferguson MK, Durkin AE (2002) Preoperative prediction of the risk of pulmonary complications after esophagectomy for cancer. J Thorac Cardiovasc Surg 123:661–669
Law S, Wong KH, Kwok KF, Chu KM, Wong J (2004) Predictive factors for postoperative pulmonary complications and mortality after esophagectomy for cancer. Ann Surg 240:791–800
Mariette C, Taillier G, Van Seuningen I, Triboulet JP (2004) Factors affecting postoperative course and survival after en-bloc resection for esophageal carcinoma. Ann Thorac Surg 78:1177–1183
Sjoquist KM, Burmeister BH, Smithers BM, Zalcberg JR, Simes RJ, Barbour A et al (2011) Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal cancer. An updated meta-analysis. Lancet Oncol 12:681–692
Haase O, Raue W, Neuss H, Koplin G, Mielitz U, Schwenk W (2013) Influence of postoperative fluid management on pulmonary function after esophagectomy. Acta Chir Belg 113:415–422
Michelet P, D’Journo XB, Roch A, Doddoli C, Marin V, Papazian L et al (2006) Protective ventilation influences systemic inflammation after esophagectomy: a randomized controlled study. Anaesthesiology 105:911–919
Cense HA, Lagarde SM, de Jong K, Omloo JM, Busch OR, Henny CP et al (2006) Association of no epidural analgesia with postoperative morbidity and mortality after transthoracic esophageal cancer resection. J Am Coll Surg 202:395–400
Bierre SSA, van Berge Henegouwen, Maas KW, Bonavina L, Rosman C, Garcia JR et al (2012) Minimally invasive versus open esophagectomy for patients with esophageal cancer: a multicentre, open-label, randomized controlled trial. Lancet 379:1887–1892
Briez N, Piessen G, Torres F, Lebuffe G, Triboulet JP, Mariette C (2012) Effects of hybrid minimally-invasive oesophagectomy on major postoperative pulmonary complications. Br J Surg 99:1547–1553
D’Journo XB, Michelet P, Papazian L, Reynaud-Gaubert M, Doddoli C, Giudicelli R et al (2008) Airway colonization and postoperative pulmonary complications after neoadjuvant therapy for esophageal cancer. Eur J Cardiothorac Surg 32:444–450
Hölscher AH, Fetzner U (2012) Modern diagnostics and stage-oriented surgery. Therapy of adenocarcinoma of the esophagogastric junction. Chirurg 83:702–708
Schröder W, Bollschweiler E, Kossow C, Hölscher AH (2006) Preoperative risk analysis—a reliable predictor of postoperative outcome after transthoracic esophagectomy? Langenbecks Arch Surg 391:455–460
Hölscher AH, Schneider PM, Gutschow C, Schröder W (2007) Laparoscopic ischemic conditioning of the stomach for esophageal replacement. Ann Surg 245:241–246
Schröder W, Hölscher AH, Bludau M, Vallböhmer D, Bollschweiler E, Gutschow C (2010) Ivor-Lewis esophagectomy with and without laparoscopic conditioning of the gastric conduit. World J Surg 34:738–743
Wittekind C, Meyer HJ (2010) TNM-Klassifikation maligner Tumoren. Wiley-VCH Verlag GmbH, Weinheim
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Bailey SH, Bull DA, Harpole DH, Rentz JJ, Neumayer LA, Pappas TN et al (2003) Outcomes after esophagectomy: a ten-year prospective cohort. Ann Thorac Surg 75:217–222
Hölscher AH, Fetzner U, Bludau M, Leers J (2011) Complications and management of complications in esophageal surgery. Zentralbl Chir 136:213
Strasberg SM, Linehan DC, Hawkins WG (2009) The accordion severity grading system of surgical complications. Ann Surg 250(2):177–186
Cabello H, Torres A, Celis R, El-Ebiary M, Puig de la Bellacasa J, Xaubet A et al (1997) Bacterial colonization of distal airways in healthy subjects and chronic lung disease: a bronchoscopic study. Eur Respir J 10:1137–1144
Ioanas M, Angrill J, Baldo X (2002) Bronchial bacterial colonization in patients with resectable lung cancer. Eur Respir J 19:326–332
Sok M, Dragas AZ, Erzen J (2002) Sources of pathogens causing pleuropulmonary infections after lung cancer resection. Eur J Cardiothorac Surg 22:23–27
Belda J, Cavalcanti M, Ferrer M, Serra M, Puig de la Bellacasa J, Canalis E et al (2005) Bronchial colonization and postoperative respiratory infections in patients undergoing lung cancer surgery. Chest 128:1571–1579
Schussler O, Alifano M, Dermine H, Strano S, Casetta A, Sepulveda S et al (2006) Postoperative pneumonia after major lung resection. Am J Respir Crit Care Med 173:1161–1169
Conflicts of interest
The authors declare that they have no competing interests.
Ethical approval
The study was approved by the Ethics Committee of the University of Cologne (Nr. 13–094). For this type of study, formal consent is not required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bludau, M., Hölscher, A.H., Bollschweiler, E. et al. Preoperative airway colonization prior to transthoracic esophagectomy predicts postoperative pulmonary complications. Langenbecks Arch Surg 400, 707–714 (2015). https://doi.org/10.1007/s00423-015-1326-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-015-1326-7