
Abstract
Purpose
According to the International Union Against Cancer (UICC), R1 is defined as the microscopic presence of tumor cells at the surface of the resection margin (RM). In contrast, the Royal College of Pathologists (RCP) suggested to declare R1 already when tumor cells are found within 1 mm of the RM. The aim of this study was to determine the significance of the RM concerning the prognosis of pancreatic ductal adenocarcinoma (PDAC).
Methods
From 2007 to 2009, 62 patients underwent a curative operation for PDAC of the pancreatic head. The relevance of R status on cumulative overall survival (OS) was assessed on univariate and multivariate analysis for both the classic R classification (UICC) and the suggestion of the RCP.
Results
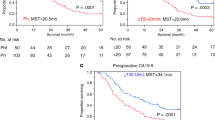
Following the UICC criteria, a positive RM was detected in 8 %. Along with grading and lymph node ratio, R status revealed a significant impact on OS on univariate and multivariate analysis. Applying the suggestion of the RCP, R1 rate rose to 26 % resulting in no significant impact on OS in univariate analysis.
Conclusions
Our study has shown that the RCP suggestion for R status has no impact on the prognosis of PDAC. In contrast, our data confirmed the UICC R classification of RM as well as N category, grading, and lymph node ratio as significant prognostic factors.




Similar content being viewed by others


References
Carpelan-Holmstrom M, Nordling S, Pukkala E, Sankila R, Luttges J, Kloppel G, Haglund C (2005) Does anyone survive pancreatic ductal adenocarcinoma? A nationwide study re-evaluating the data of the Finnish Cancer Registry. Gut 54:385–387
Sperti C, Pasquali C, Piccoli A, Pedrazzoli S (1997) Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg 21:195–200
Alexakis N, Halloran C, Raraty M, Ghaneh P, Sutton R, Neoptolemos JP (2004) Current standards of surgery for pancreatic cancer. Br J Surg 91:1410–1427
Esposito I, Kleeff J, Bergmann F, Reiser C, Herpel E, Friess H, Schirmacher P, Buchler MW (2008) Most pancreatic cancer resections are R1 resections. Ann Surg Oncol 15:1651–1660
Menon KV, Gomez D, Smith AM, Anthoney A, Verbeke CS (2009) Impact of margin status on survival following pancreatoduodenectomy for cancer: the Leeds Pathology Protocol (LEEPP). HPB (Oxford) 11:18–24
Verbeke CS (2008) Resection margins and R1 rates in pancreatic cancer—are we there yet? Histopathology 52:787–796
Butturini G, Stocken DD, Wente MN, Jeekel H, Klinkenbijl JH, Bakkevold KE, Takada T, Amano H, Dervenis C, Bassi C, Buchler MW, Neoptolemos JP (2008) Influence of resection margins and treatment on survival in patients with pancreatic cancer: meta-analysis of randomized controlled trials. Arch Surg 143:75–83, discussion 83
Verbeke CS, Leitch D, Menon KV, McMahon MJ, Guillou PJ, Anthoney A (2006) Redefining the R1 resection in pancreatic cancer. Br J Surg 93:1232–1237
Sobin LH, Gospodarowicz MK, Wittekind C (2009) International Union Against Cancer TNM classification of malignant tumours, 7th edn. Wiley-Blackwell, Oxford
The Royal College of Pathologists (2002) Standards and minimum datasets for reporting cancers. Minimum datasets for the histopathological reporting of pancreatic, ampulla of Vater and bile duct carcinoma. The Royal College of Pathologists, London
Nagtegaal ID, Marijnen CA, Kranenbarg EK, van de Velde CJ, van Krieken JH (2002) Circumferential margin involvement is still an important predictor of local recurrence in rectal carcinoma: not one millimeter but two millimeters is the limit. Am J Surg Pathol 26:350–357
Wibe A, Rendedal PR, Svensson E, Norstein J, Eide TJ, Myrvold HE, Soreide O (2002) Prognostic significance of the circumferential resection margin following total mesorectal excision for rectal cancer. Br J Surg 89:327–334
Chang DK, Johns AL, Merrett ND, Gill AJ, Colvin EK, Scarlett CJ, Nguyen NQ, Leong RW, Cosman PH, Kelly MI, Sutherland RL, Henshall SM, Kench JG, Biankin AV (2009) Margin clearance and outcome in resected pancreatic cancer. J Clin Oncol 27:2855–2862
Compton CC (2005) College of American Pathologists. Leeds Protocol. http://www.Cap.Org/apps/docs/cancer_protocols/2005/pancreasexo05_pw.Doc
Tannapfel A (2010) [Pancreatic cancer. Molecular and surgical pathology]. Pathologe 31(Suppl 2):225–228
Kloppel G, Hruban RH, Longnecker DS (2000) Ductal adenocarcinoma of the pancreas. In: Hamilton SR, Aaltonen LA (eds) WHO classification of tumours: pathology and genetics of tumours of the digestive system. IARC, Lyon, pp 221–230
Pedrazzoli S, DiCarlo V, Dionigi R, Mosca F, Pederzoli P, Pasquali C, Kloppel G, Dhaene K, Michelassi F (1998) Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Lymphadenectomy Study Group. Ann Surg 228:508–517
Kayahara M, Nagakawa T, Ueno K, Ohta T, Takeda T, Miyazaki I (1993) An evaluation of radical resection for pancreatic cancer based on the mode of recurrence as determined by autopsy and diagnostic imaging. Cancer 72:2118–2123
Kurahara H, Takao S, Maemura K, Shinchi H, Natsugoe S, Aikou T (2007) Impact of lymph node micrometastasis in patients with pancreatic head cancer. World J Surg 31:483–490, discussion 91–2
Albores-Saavedra J, Heffess C, Hruban RH, Klimstra D, Longnecker D (1999) Recommendations for the reporting of pancreatic specimens containing malignant tumors. The Association of Directors of Anatomic and Surgical Pathology. Am J Clin Pathol 111:304–307
Kleeff J, Reiser C, Hinz U, Bachmann J, Debus J, Jaeger D, Friess H, Buchler MW (2007) Surgery for recurrent pancreatic ductal adenocarcinoma. Ann Surg 245:566–572
Campbell F, Smith RA, Whelan P, Sutton R, Raraty M, Neoptolemos JP, Ghaneh P (2009) Classification of R1 resections for pancreatic cancer: the prognostic relevance of tumour involvement within 1 mm of a resection margin. Histopathology 55:277–283
Westgaard A, Tafjord S, Farstad IN, Cvancarova M, Eide TJ, Mathisen O, Clausen OP, Gladhaug IP (2008) Resectable adenocarcinomas in the pancreatic head: the retroperitoneal resection margin is an independent prognostic factor. BMC Cancer 8:5
Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Buchler MW (2004) Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. Br J Surg 91:586–594
Howard TJ, Krug JE, Yu J, Zyromski NJ, Schmidt CM, Jacobson LE, Madura JA, Wiebke EA, Lillemoe KD (2006) A margin-negative R0 resection accomplished with minimal postoperative complications is the surgeon's contribution to long-term survival in pancreatic cancer. J Gastrointest Surg 10:1338–1345, discussion 45–6
Jarufe NP, Coldham C, Mayer AD, Mirza DF, Buckels JA, Bramhall SR (2004) Favourable prognostic factors in a large UK experience of adenocarcinoma of the head of the pancreas and periampullary region. Dig Surg 21:202–209
Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, Hodgin MB, Sauter PK, Hruban RH, Riall TS, Schulick RD, Choti MA, Lillemoe KD, Yeo CJ (2006) 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg 10:1199–1210, discussion 210–1
Raut CP, Tseng JF, Sun CC, Wang H, Wolff RA, Crane CH, Hwang R, Vauthey JN, Abdalla EK, Lee JE, Pisters PW, Evans DB (2007) Impact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann Surg 246:52–60
Hernandez J, Mullinax J, Clark W, Toomey P, Villadolid D, Morton C, Ross S, Rosemurgy A (2009) Survival after pancreaticoduodenectomy is not improved by extending resections to achieve negative margins. Ann Surg 250:76–80
Perini MV, Montagnini AL, Jukemura J, Penteado S, Abdo EE, Patzina R, Cecconello I, Cunha JE (2008) Clinical and pathologic prognostic factors for curative resection for pancreatic cancer. HPB (Oxford) 10:356–362
Brennan MF, Kattan MW, Klimstra D, Conlon K (2004) Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann Surg 240:293–298
Cameron JL, Crist DW, Sitzmann JV, Hruban RH, Boitnott JK, Seidler AJ, Coleman J (1991) Factors influencing survival after pancreaticoduodenectomy for pancreatic cancer. Am J Surg 161:120–124, discussion 24–5
Kuhlmann KF, de Castro SM, Wesseling JG, ten Kate FJ, Offerhaus GJ, Busch OR, van Gulik TM, Obertop H, Gouma DJ (2004) Surgical treatment of pancreatic adenocarcinoma; actual survival and prognostic factors in 343 patients. Eur J Cancer 40:549–558
Meyer W, Jurowich C, Reichel M, Steinhauser B, Wunsch PH, Gebhardt C (2000) Pathomorphological and histological prognostic factors in curatively resected ductal adenocarcinoma of the pancreas. Surg Today 30:582–587
Nakao A, Takeda S, Sakai M, Kaneko T, Inoue S, Sugimoto H, Kanazumi N (2004) Extended radical resection versus standard resection for pancreatic cancer: the rationale for extended radical resection. Pancreas 28:289–292
Hartwig W, Hackert T, Hinz U, Gluth A, Bergmann F, Strobel O, Buchler MW, Werner J (2011) Pancreatic cancer surgery in the new millennium: better prediction of outcome. Ann Surg 254:311–319
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Additional information
MS Janot and S Kersting contributed equally.
Rights and permissions
About this article
Cite this article
Janot, M.S., Kersting, S., Belyaev, O. et al. Can the new RCP R0/R1 classification predict the clinical outcome in ductal adenocarcinoma of the pancreatic head?. Langenbecks Arch Surg 397, 917–925 (2012). https://doi.org/10.1007/s00423-012-0953-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-012-0953-5