
Abstract
Background and aim
Mesh usage in repair of acutely incarcerated hernia is still a concern owing to infectious complications. The aim of this prospective clinical observational cohort study was to evaluate factors that increase the risk of bowel necrosis and to document the clinical outcome of the patients with acutely incarcerated groin hernias treated by non-absorbable mesh.
Materials and methods
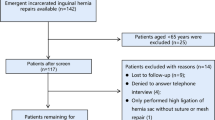
Ninety-five adult patients with acutely incarcerated groin hernias who underwent prosthetic herniorrhaphy from 1997 to 2005 were prospectively included. The patients were evaluated in two groups, which were based on whether the bowel resection was required (group 1) or not (group 2). Demographics and characteristics of patients in each group were compared. Chi-square, Fisher’s exact, and Mann–Whitney U test were used to determine the statistical significance (p < 0.05).
Results
Bowel resection was required in 14 (14.7%) and not required in 81 (85.3%) patients. Duration of symptoms longer than 6 h was an important factor for determining the need for resection (p = 0.026). No significant difference was noted concerning the development of wound infection, postoperative recurrence, morbidity, and mortality rates between the two groups.
Conclusions
Our results suggest that duration of symptoms longer than 6 h was an important factor for determining the need for resection. The use of non-absorbable mesh for acutely incarcerated groin hernia repair is effective and may be used with an acceptable incidence of wound infection and recurrence even when intestinal necrosis was present.
Similar content being viewed by others

References
Pans A, Desaive C, Jaquet N (1997) Use of a preperitoneal prosthesis for strangulated groin hernia. Br J Surg 84:310–312 doi:10.1002/bjs.1800840307
Wysocki A, Pozniczek M, Krzywon J et al (2001) Use of polypropylene prostheses for strangulated inguinal and incisional hernias. Hernia 5:105–106 doi:10.1007/s100290100013
Wysocki A, Kulawik J, Poźniczec M et al (2006) Is the Lichtenstein operation of strangulated groin hernia a safe procedure. World J Surg 30:2065–2070 doi:10.1007/s00268-005-0416-z
Kurt N, Oncel M, Ozkan Z et al (2003) Risk and outcome of bowel resection in patients with incarcerated groin hernias: Retrospective study. World J Surg 27:741–743 doi:10.1007/s00268-003-6826-x
Rai S, Chandra SS, Smile SR (1998) A study of the risk of strangulation and obstruction in groin hernias. Aust N Z J Surg 68:650–654 doi:10.1111/j.1445-2197.1998.tb04837.x
Kulah B, Kulacoglu IH, Oruc MT et al (2001) Presentation and outcome of incarcerated external hernias in adults. Am J Surg 181:101–104 doi:10.1016/S0002-9610(00)00563-8
Bekoe S (1973) Prospective analysis of the management of incarcerated and strangulated inguinal hernias. Am J Surg 126:665–668 doi:10.1016/S0002-9610(73)80018-2
Brasso K, Nielsen KL, Christiansen J (1989) Long-term results of surgery for incarcerated groin hernia. Acta Chir Scand 155:583–585
Read CR (2001) Metabolic aspects of hernia disease. In: Bendavid R (ed) Abdominal wall hernias: principles and management. Springer, New York, pp 139–142
Andrews NJ (1981) Presentation and outcome of strangulated external hernia in a district general hospital. Br J Surg 68:329–332 doi:10.1002/bjs.1800680513
Hachisuka T (2003) Femoral hernia repair. Surg Clin North Am 83:1189–1205 doi:10.1016/S0039-6109(03)00120-8
Oishi SN, Page CP, Schwesinger WH (1991) Complicated presentations of groin hernias. Am J Surg 162:568–571 doi:10.1016/0002-9610(91)90110-Y
Ohene-Yeboah M (2003) Strangulated external hernias in Kumasi. West Afr J Med 22:310–313
Bessa SS, Katri KM, Abdel-Salam WN et al (2007) Early results from the use of the Lichtenstein repair in the management of strangulated groin hernia. Hernia 11:239–242 doi:10.1007/s10029-007-0207-6
Campanelli FM, Nicolosi FM, Pettinari D et al (2004) Prosthetic repair, intestinal resection, and potentially contaminated areas: safe and feasible. Hernia 8:190–192 doi:10.1007/s10029-004-0242-5
Lavonius MI, Ovaska J (2000) Laparoscopy in the evaluation of the incarcerated mass in groin hernia. Surg Laparosc Endosc 14:488–489
Lin E, Wear K, Tiszenkel HI (2002) Planned reduction of incarcerated groin hernias with hernia sac laparoscopy. Surg Endosc 16:936–938 doi:10.1007/s00464-001-8242-3
Franklin ME Jr, Gonzalez JJ Jr, Michaelson RP et al (2002) Preliminary experience with new bioactive prosthetic material for repair of hernias in infected fields. Hernia 6:171–174 doi:10.1007/s10029-002-0078-9
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Atila, K., Guler, S., Inal, A. et al. Prosthetic repair of acutely incarcerated groin hernias: a prospective clinical observational cohort study. Langenbecks Arch Surg 395, 563–568 (2010). https://doi.org/10.1007/s00423-008-0414-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-008-0414-3