
Abstract
Background
The necessary extent of thyroid resection in benign nodular goiter is under debate. The aim of our study was to compare the long-term outcome of different thyroid resection modes with special interest in the incidence of recurrent nodules and the use of oral thyroid hormone medication.
Materials and methods
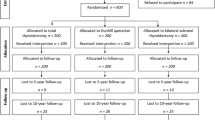
We performed a follow-up examination of 109 patients (23 men and 86 women) having been operated for benign nodular goiter at our department 10 years ago. Unilateral resections and function-preserving resections of at least one thyroid lobe were classified as function-preserving (FP). Total thyroidectomy, Dunhill’s operation and bilateral subtotal thyroidectomy were rated as standard-radical (STR). On follow-up, we recorded current oral thyroid hormone medication, thyroid function tests and ultrasound of the neck.
Results
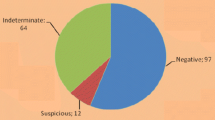
Seventy-three patients had FP resection (67%), while 36 were STR-operated (33%). The subsequent medical treatment was performed by dedicated endocrinologists (n = 19), internists (n = 11) or primary-care physicians (n = 59). Twenty patients had no medical attendance. Recurrent nodules were found in 13 cases in the FP group (18.6%) vs. 3 cases in the STR group (2.5%; p < 0.001). In both groups, about 80% of patients used thyroid hormone medication 10 years after operation.
Conclusion
There was no advantage in thyroid function tests nor lesser medication in the FP group. The risk for recurrent nodules was significantly higher in the FP than in the STR-operated patients.
Similar content being viewed by others

References
Gemsenjager E (1993) Goiter surgery from Kocher to today. Schweiz Med Wochenschr 123(6):207–213 13
Harness JK (1986) Total thyroidectomy: complications and technique. World J Surg 10:781–786
Liu Q (1998) Total thyroidectomy for benign thyroid disease. Surgery 123:2–7
Reeve TS (1987) Total thyroidectomy: the preferred option for multinodular goiter. Ann Surg 206:782–786
Csaky G (2002) Early results after minimal lobectomy for benign nodular goiter. Magy Seb 55(4):268–271
Delbridge L (1992) Total thyroidectomy: the technique of capsular dissection. Aust N Z J Surg 62:96–99
Delbridge L (1999) Total thyroidectomy for bilateral benign multinodular goiter: effect of changing practice. Arch Surg 134:1389–1393
Gemsenjager E (1993) Goiter surgery from Kocher to today. Schweiz Med Wochenschr 123(6):207–213 13
Koyuncu A (2003) Comparison of different thyroidectomy techniques for benign thyroid disease. Endocrine J 50(6):723–727
La Gamma A (1994) Predictive factors of nodular recurrence after thyroidectomy for goiter. J Chir 131(2):66–72
Muller PE (2001) Indications, risks and acceptance of total thyroidectomy for multinodular benign goiter. Surg Today 31(11):998–962
Reichmann I (1998) Results of selective goiter resection in functional autonomy. Zentralbl Chir 123(1):34–38
Gomez PA (2006) Development and outcomes of the surgical management of multinodular goiter. Cir Esp 80(2):83–89
Ayache S (2005) Evolution of the thyroid surgical treatment to the total thyroidectomy. Ann Otolaryngol Chir Cervicofac 122(3):127–133 (Jun)
Ozbas S (2005) Comparison of the complications of subtotal, near total and total thyroidectomy in the surgical management of multinodular goiter. Endocr J 52(2):199–205
Siragusa G (1998) Subtotal thyroidectomy or total thyroidectomy in the treatment of benign thyroid disease. Our experience. Minerva Chir 53(4):233–238
Peix JL (1996) Role of total thyroidectomy in the treatment of benign thyroid diseases. Ann Endocrinol 57(6):502–507
Bron LP (2004) Total thyroidectomy for clinically benign disease of the thyroid gland. Br J Surg 91(5):569–574
Marchesi M (2002) High rate of recurrence after lobectomy for solitary thyroid nodule. Eur J Surg 168(7):397–400
Thomusch O (2003) Is primary total thyroidectomy justified in benign multinodular goiter? Results of a prospective quality assurance study of 45 hospitals offering different levels of care. Chirurg 74:437–443
Farkas EA (2002) A comparison of total thyroidectomy and lobectomy in the treatment of dominant thyroid nodules. Am Surg 68(8):678–782
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lehwald, N., Cupisti, K., Willenberg, H.S. et al. Standard-radical vs. function-preserving surgery of benign nodular goiter—a sonographic and biochemical 10-year follow-up study. Langenbecks Arch Surg 394, 279–283 (2009). https://doi.org/10.1007/s00423-008-0328-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-008-0328-0