
Abstract
Background
Laparoscopic resection of the sigmoid colon is generally considered as feasible option to open surgery, but standardised guidelines on surgical details have not been adopted yet. The aim of this survey was to investigate which techniques were applied by laparoscopic surgeons who are members of the Surgical Working Group for Minimal Invasive Surgery (CAMIC) of the German Surgical Society.
Materials and methods
In 2005, we conducted a written survey among all members of the CAMIC asking them for their routine surgical strategy of laparoscopic sigmoid resection in a standardised multiple-choice questionnaire. This questionnaire consisted of 20 questions covering main technical issues of laparoscopic sigmoid resection including trocar and team positioning, mobilisation and resection of the left colon, specimen retrieval as well as anastomosing technique. The results were classified into four levels of consensus depending on the level of agreement between participating surgeons.
Results
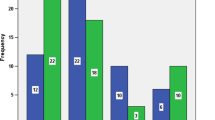
There were 292 surgeons who took part in the survey. Strong consensus (>95% agreement) was only found in 1 of 20 technical details: the operating surgeon standing at the patient right’s side. Consensus (75–95% agreement) was found for: position of the first assistant standing to the patient’s left side, size of the camera port is 10 mm, lateral mobilisation of the left hemicolon before ligating the inferior mesenteric artery, extracorporeal resection of the sigmoid via minilaparotomy, transrectal stapling of the colorectal anastomosis, intraoperative testing of the anastomosis for leakage, no regular suturing over the anastomosis and irrigating of the abdominal cavity after surgery.
Conclusions
Variability of technical details of laparoscopic sigmoidectomy was surprisingly high among German laparoscopic surgeons. This fact should be considered when discussing clinical studies about laparoscopic sigmoidectomy because trocar position, type of minilaparotomy and dissection techniques may very well influence patient outcome after laparoscopic surgery. Therefore, publications of clinical results concerning laparoscopic sigmoid resection should include a precise description of the technical details of the operation.
Similar content being viewed by others

References
Jacobs M, Verdeja JC, Goldstein HS (1991) Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1(3):144–150
Fowler DL, White SA, Anderson CA (1995) Laparoscopic colon resection: 60 cases. Surg Laparosc Endosc 5(6):468–471
Rose J, Schneider C, Yildirim C, Geers P, Scheidbach H, Kockerling F (2004) Complications in laparoscopic colorectal surgery: results of a multicentre trial. Tech Coloproctology 8(Suppl 1):25–28
Scheidbach H, Schneider C, Huegel O, Barlehner E, Konradt K, Wittekind C, Kockerling F (2002) Laparoscopic sigmoid resection for cancer: curative resection and preliminary medium-term results. Dis Colon Rectum 45(12):1641–1647
Kockerling F, Rose J, Schneider C, Scheidbach H, Scheuerlein H, Reymond MA et al (1999) Laparoscopic colorectal anastomosis: risk of postoperative leakage. Results of a multicenter study. Laparoscopic Colorectal Surgery Study Group (LCSSG). Surg Endosc 13(7):639–644
Kockerling F, Schneider C, Reymond MA, Scheidbach H, Scheuerlein H, Konradt J et al (1999) Laparoscopic resection of sigmoid diverticulitis. Results of a multicenter study. Laparoscopic Colorectal Surgery Study Group. Surg Endosc 13(6):567–571
Schlachta CM, Mamazza J, Gregoire R, Burpee SE, Poulin EC (2003) Could laparoscopic colon and rectal surgery become the standard of care? A review and experience with 750 procedures. Can J Surg 46(6):432–440
Bergamaschi R, Arnaud JP (1997) Intracorporeal colorectal anastomosis following laparoscopic left colon resection. Surg Endosc 11(8):800–801
Sigel A, Zerz A, Molle B, Knaus J, Zund M et al (2004) Medial mobilisation of the left hemicolon. Chirurg 75(6):605–608
Hackert T, Uhl W, Buchler MW (2002) Specimen retrieval in laparoscopic colon surgery. Dig Surg 19(6):502–506
Nelson H, Petrelli N, Carlin A, Couture J, Fleshman J, Guillem J, Miedema B et al (2001) Guidelines 2000 for colon and rectal cancer surgery. J Natl Cancer Inst 93(8):583–596
Veldkamp R, Gholghesaei M, Bonjer HJ, Meijer DW, Buunen M, Jeekel J et al (2004) Laparoscopic resection of colon cancer: consensus of the European Association of Endoscopic Surgery (EAES). Surg Endosc 18(8):1163–1185
Milsom JW, Böhm B (1996) Laparoscopic colorectal surgery. Springer, Berlin Heidelberg New York
Milsom JW, Böhm B, Nakajima K (2006) Laparoscopic colorectal surgery. Springer, Berlin Heidelberg New York
Köhler L, Sauerland S, Neugebauer E (1999) Diagnosis and treatment of diverticular disease. Results of a consensus development conference (EAES). Surg Endosc 13:430–436
Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS (1996) Evidence based medicine: what it is and what it isn’t. BMJ 312(7023):71–72
Hoffmann JC, Fischer I, Hohne W, Zeitz M, Selbmann HK (2004) Methodological basis for the development of consensus recommendations. Z Gastroenterol 42(9):984–986
Schwenk W, Haase O, Neudecker J, Muller JM (2005) Short term benefits for laparoscopic colorectal resection. Cochrane Database Syst Rev 20(3):CD003145
Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, Visa J (2002) Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 359(9325):2224–2229
Braga M, Frasson M, Vignali A, Zuliani W, Civelli V, Di Carlo V (2005) Laparoscopic vs. open colectomy in cancer patients: long-term complications, quality of life, and survival. Dis Colon Rectum 48(12):2217–2223
Leung KL, Kwok SP, Lam SC, Lee JF, Yiu RY, Ng SS, Lai PB, Lau WY (2004) Laparoscopic resection of rectosigmoid carcinoma: prospective randomised trial. Lancet 363(9416):1187–1192
Clinical Outcomes of Surgical Therapy Study Group (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350(20):2050–2059
Senagore AJ (2005) Laparoscopic sigmoid colectomy for diverticular disease. Surg Clin North Am 85(1):19–24
Kum CK, Eypasch E, Aljaziri A, Troidl H (1996) Randomized comparison of pulmonary function after the ‘French’ and ‘American’ techniques of laparoscopic cholecystectomy. Br J Surg 83:938–941
Bisagaard T, Klarskov B, Trap R, Kehlet H, Rosenberg J (2000) Pain after microlaparoscopic cholecystectomy. Surg Endosc 14:340–344
Schwenk W, Neudecker J, Mall J, Böhm B, Müller JM (2000) Prospective randomised, blinded trial of pulmonary function, pain, and cosmetic result after laparoscopic vs. microlaparoscopic cholecystectomy. Surg Endosc 14 (345):348
Liang JT, Lai HS, Huang KC, Chang KJ, Shieh MJ, Jeng YM, Wang SM (2003) Comparison of medial-to-lateral versus traditional lateral-to-medial laparoscopic dissection sequences for resection of rectosigmoid cancers: randomized controlled clinical trial. World J Surg 27(2):190–196
Petrowsky H, Demartines N, Rousson V, Clavien PA (2004) Evidence-based value of prophylactic drainage in gastrointestinal surgery. A systematic review and meta-analyses. Ann Surg 240:1074–1085
Adams AS, Soumerai SB, Lomas J, Ross-Degnan D (1999) Evidence of self-report bias in assessing adherence to guidelines. Int J Qual Health Care 11(3):187–192
Acknowledgment
We would like to thank Prof. Dr. med. Bittner and Prof. Dr. med. Köckerling for providing us with the contact of CAMIC members.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Neudecker, J., Bergholz, R., Junghans, T. et al. Laparoscopic sigmoidectomy in Germany—a standardised procedure?. Langenbecks Arch Surg 392, 573–579 (2007). https://doi.org/10.1007/s00423-007-0172-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-007-0172-7