
Abstract
Background
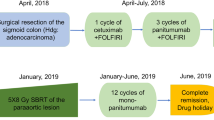
Organ transplantation is a standard procedure today. Due to immunosuppressive drugs and increasing survival after organ transplantation, patients with transplanted organs carry an increased risk of developing malignant tumours. Accordingly, more patients with malignant tumours after transplantation will be faced by general or oncology surgeons. We report the case of a 48-year-old patient with advanced rectal cancer 6.5 years after pancreas–kidney-transplantation for type I diabetes.
Method
The patient was treated with neo-adjuvant radio-chemotherapy, followed by low anterior rectal resection with total mesorectal excision. Consecutively, a solitary hepatic metastasis, a solitary pulmonary metastasis and a chest wall metastasis were resected over the course of 13 months.
Result
The patient eventually died of metastasized cancer 32 months after therapy had been initiated, his organ grafts functioning well until his death.
Conclusion
Our case report provides evidence that transplantation patients should receive standard oncology treatment, including neo-adjuvant treatment, so long as their general condition and organ graft functions allow us to do so, although a higher degree of morbidity might be encountered.



Similar content being viewed by others

References
Sutherland DE, Gruessner RWG, Dunn DL, Matas A, Humar A, Kandaswamy R, Mauer SM, Kennedy WR, Goetz FC, Robertson RP, Gruessner AC, Najarian JS (2001) Lessons learned from more than 1000 pancreas transplants at a single institution. Ann Surg 233:463–501
Pirson Y, Vandeleene B, Squifflet JP (2000) Kidney and kidney–pancreas transplantation in diabetic recipients. Diabetes Metab 26 [Suppl 4]:86–89
Hopt UT, Benz S, Pfeffer F, Schareck W, Irkin I, Busing M (1994) Simultaneous pancreas/kidney transplantation—the optimal therapy for the type I diabetics with end-stage renal disease in Europe, too? Transpl Int 7 [Suppl 1]:S414–S416
Sheiner PA, Magliocca JF, Bodian CA, Kim-Schluger L, Altaca G, Guarrera JV, Emre S, Fishbein TM, Guy SR, Schwartz ME, Miller CM (2000) Long-term medical complications in patients surviving >or = 5 years after liver transplant. Transplantation 69:781–789
Kishikawa H, Ichikawa Y, Yazawa K, Hanafusa T, Fukunishi T, Ebisui C, Okuyama A, Nagano S (1998) Malignant neoplasm in kidney transplantation. Int J Urol 5:521–525
Stewart T, Tsai SCJ, Grayson H, Henderson R, Opelz G (1995) Incidence of de-novo breast cancer in women chronically immunosuppressed after organ transplantation. Lancet 346:796–798
Schmähl D, Penn I (1991) Cancer in organ transplant recipients. In: Schmähl D, Penn I (eds) Organ transplantation. Springer, Heidelberg, pp 19–27
Herman M, Weinstein T, Korsets A, Chagnac A, Ori Y, Zevin D, Malachi T, Gafter U (2001) Effect of cyclosporin A on DNA repair and cancer incidence in kidney transplant recipients. J Lab Clin Med 137:14–20
Euvrard S, Kanitakis J, Claudy A (2003) Skin cancers after organ transplantation. N Engl J Med 348:1681–1691
Penn I (1993) Neoplastic complications of transplantation. Semin Respir Infect 8:233–239
Penn I (1993) Incidence and treatment of neoplasia after transplantation. J Heart Lung Transpl 12:S328–S336
Kyllonen L, Salmela K, Pukkala E (2000) Cancer incidence in a kidney-transplanted population. Transpl Int 13 [Suppl 1]:S394–S398
Birkeland SA (1997) De novo cancers complicating renal transplantation: experience in the Nordic countries. Ann Transplant 2:22–26
Kapiteijn E, Marijnen CAM, Nagtegaal ID, Putter H, Steup WH, Wiggers T, Rutten HJ, Pahlman L, Glimelius B, van Krieken JH, Leer JW, van de Velde CJ (2001) Preoperative radiotherapy combined with total mesorectal excision for the resectable rectal cancer. N Eng J Med 345:638–646
Rau B, Hohenberger P, Gellermann J, Hunerbein M, Hildebrandt B, Schneider U, Riess H, Wust P, Schlag PM (2002) T4 Rektumkarzinom. Operative and multimodal therapy. Chirurg 73:147–153
Stangl R, Altendorf-Hofmann A, Charnley RM, Scheele J (1994) Factors influencing the natural history of colorectal liver metastases. Lancet 343:1405–1410
Lutz J, Heemann U (2003) Tumours after kidney transplantation. Curr Opin Urol 13:105–109
Jacobsohn DA, Vogelsang GB (2002) Novel pharmacotherapeutic approaches to prevention and treatment of GVHD. Drugs 62:879–889
Witzigmann H, Rhein T, Geissler F, Thiery J, Serr F, Tannapfel A, Uhlmann D, Metzner R, Hauss J (2002) Immunosuppression with sirolimus/tacrolimus combination in pancreas transplantation: 1-year results. Transplant Proc 34:3354–3356
Guba M, von Breitenbuch P, Steinbauer M, Koehl G, Flegel S, Hornung M, Bruns CJ, Zuelke C, Farkas S, Anthuber M, Jauch K-W, Geissler EK (2002) Rapamycin inhibits primary and metastatic tumor growth by antiangiogenesis: involvement of vascular endothelial growth factor. Nat Med 8:128–135
Luan FL, Ding R, Sharma VK, Chon WJ, Lagman M, Suthanthiran M (2003) Rapamycin is an effective inhibitor of human renal cancer metastasis. Kidney Int 63:917–926
Starzl TE, Murase N, Abu-Elmagd K, et al (2003) Tolerogenic immuno-suppression for organ transplantation. Lancet 361:1502–1510
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zittel, T.T., Mehl, C.F.R., Reichmann, U. et al. Treatment of advanced rectal cancer in a patient after combined pancreas–kidney transplantation. Langenbecks Arch Surg 389, 6–10 (2004). https://doi.org/10.1007/s00423-003-0422-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-003-0422-2