
Abstract
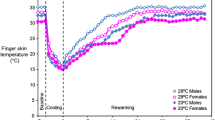
Objective: Frequent use of vibrating tools may lead to typical attacks of Raynaud’s phenomenon (RP). The present study assesses the feasibility of the use of thermographic measurements of blood rheometry in the diagnosis of vibration-induced white-finger (VWF) syndrome. Subjects and methods: We studied 38 patients that were suffering from RP (primary RP, n=29; VWF, n=9) and 13 controls (six men and 45 women; mean age 49.1±11.6 years). Superficial finger skin blood flow was assessed with an infrared thermocamera before and after exposure to heat and cold. Fibrinogen, whole-blood viscosity and erythrocyte aggregation at different shear rates and plasma viscosity were measured. Main results: In patients with RP finger temperatures after re-warming were lower than those in controls [right hand digit (DIG) I P<0.02; DIG II–V P<0.01; left hand DIG I P<0.01; DIG II-V p<0.02], male patients with primary RP had higher Fg-values (P<0.02) and a trend to higher plasma viscosity. Patients with VWF had a trend to lower plasma viscosity than controls. Whole-blood viscosity at each shear rate was highest in patients with VWF. Conclusion: Provocation manoeuvres are essential in the diagnosis of RP. We speculate that the decreased plasma viscosity in VWF is a compensatory physiological mechanism, probably counteracting the chronic effects of vasospasm. The rise in whole-blood viscosity could be due to endothelial injury or to a reduction in the venous blood pH level. The abnormal cold reactivity of patients with RP may be partly related to rheological factors.
Similar content being viewed by others

References
Alexander GSM, Blake DR, Holman RL, Bacon PA (1981) Predictive value of paired plasma and serum viscosity in early rheumatic conditions. BMJ 282:1198
Boccalon HJ, Marguery MC, Ginestet MC, Puel PF (1987) Laser Doppler flowmetry and standardized thermal test in normals and Raynaud’s phenomenon. Int Angiol 6:107–118
Coughlin P, Chetter IC, Kent PJ, Kester RC (1999) Vascular Surgical Society of Great Britain and Ireland: analysis of cold provocation thermography in the objective diagnosis of the hand–arm vibration syndrome. Br J Surg 86:694–695
Darton K, Black CM (1990) The use of infra-red thermography in a rheumatology unit. Br J Rheumatol 29:291–292
Ekenvall L, Lindblad LE, Carlsson A, Etzell BM (1988) Afferent and efferent nerve injury in vibration white fingers. J Auton Nerv Syst 24:261–266
Greenstein D, Kester RC (1997) The hemorheologic effects of hand-transmitted vibration. Angiology 48:813–819
Griffin MJ, Bovenzi M (2002) The diagnosis of disorders caused by hand-transmitted vibration: Southampton Workshop 2000. Int Arch Occupational Environ Health 75:1–5
Lacombe C, Mouthon JM, Bucherer C, Lelievre JC, Bletry O, Godeau P (1992) Raynaud’s phenomenon and blood viscosity. J Mal Vasc 17:132–135
Larkin JG, Lowe GD, Sturrock RD, Forbes CD (1984) The relationship of plasma and serum viscosity to disease activity and smoking habit in rheumatoid arthritis. Br J Rheumatol 23:15–19
Noel B (2000) Pathophysiology and classification of the vibration white finger. Int Arch Occupational Environ Health 73:150–155
Okada A, Inaba R, Furono T, Nohara S, Ariizumi M (1987) Usefulness of blood parameters, especially viscosity, for the diagnosis and elucidation of pathogenetic mechanisms of the hand–arm vibration syndrome. Scand J Work Environ Health 13:358–362
Olsen N (2002) Diagnostic aspects of vibration-induced white finger. Int Arch Occupational Environ Health 75:6–13
Pelmear P, Kusiak R (1994) Clinical assessment of the hand–arm vibration syndrome. Nagoya J Med Sci 57:27–41
Sandhagen B, Wegener T (1985) Blood viscosity and finger systolic pressure in primary and traumatic vasospastic disease. Ups J Med Sci 90:55–59
Stoyneva Z, Lyapima M, Tzvetkov D, Vodenicharov E (2003) Current pathophysiological views on vibration-induced Raynaud’s phenomenon. Cardiovasc Res 57:615–624
Toren K, Berg M, Gudmundsson M, Tarkowski A (1992) Rheological and immunological findings in dockers with vibration-induced white fingers. Int Arch Occupational Environmental Health 64:71–73
Von Bierbrauer A, Schilk I, Lucke C, Schmidt JA (1998) Infrared thermography in the diagnosis of Raynaud’s phenomenon in vibration-induced white finger. Vasa 27:994
Wichers G, Smit AJ, van der Meer J, Wouda AA, Halie MR (1992) Rheological properties of blood in Raynaud’s phenomenon. Vasa Suppl 34:29–33
Windberger U, Bartholovitsch A, Plasenzotti R, Korak KJ, Heinze G (2003) Whole blood viscosity, plasma viscosity and erythrocyte aggregation in nine mammalian species: reference values and comparison of data. Exp Physiol 88:431–440
Ziegler S, Brunner M, Eigenbauer E, Minar E (2003) Long-term outcome of primary Raynaud’s phenomenon and its conversion to connective tissue disease: a 12-year retrospective patient analysis. Scand J Rheumatol 32:343–347
Ziegler S, Gschwandtner M, Zoch C, Barth A, Minar E, Rudiger H, Osterode W (2004) Laser Doppler anemometry distinguishes primary Raynaud phenomenon from VWF syndrome. Microvasc Res 68:203–208
Acknowledgments
The study was financially supported by the”Jubiläumsfond” of the Austrian Nationalbank
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ziegler, S., Zöch, C., Gschwandtner, M. et al. Thermoregulation and rheological properties of blood in primary Raynaud’s phenomenon and the vibration-induced white-finger syndrome. Int Arch Occup Environ Health 78, 218–222 (2005). https://doi.org/10.1007/s00420-004-0601-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-004-0601-7