
Abstract
Purpose
To compare the significance of white-on-white standard automated perimetry (SAP), matrix frequency doubling technology (FDT), and flicker-defined form perimetry (FDF) for early detection of nerve fiber layer loss in early glaucoma patients.
Methods
Fifty-one healthy controls and 40 patients with early glaucomatous nerve fiber loss were enrolled in this study. Patients had retinal nerve fiber layer (RNFL) imaging and visual field testing by SAP, FDT matrix, and FDF perimetry at the same visit. Visual field defects were confirmed with two or more consecutive examinations by the same types of perimetry. Significant retinal nerve fiber layer loss and thus early glaucoma was defined with the reference to the RNFL thickness deviation map. The sensitivity, specificity, correlation, MD (mean deviation) and PSD (pattern standard deviation) visual field indexes, and area under the receiver operating characteristic curve (AUC) of MD and PSD of the perimetries were compared.
Results
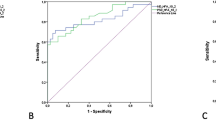
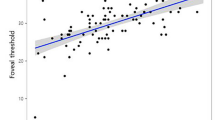
There was a significant difference in nerve fiber layer thickness between healthy patients (97.7 ± 1.34 μm and patients with early glaucoma (84.1 ± 1.58 μm) (p < 0.001). Taking all patients with early glaucoma into consideration, the sensitivity was highest for FDF perimetry (87 %), followed by FDT matrix (62.5 %), and then SAP (40 %). The specificity was 69.2 % for SAP, 62.8 % for FDT matrix, and 38.4 % for FDF perimetry. MD (mean deviation) and PSD (pattern standard deviation) in FDF and FDT matrix were significantly different between patients with RNFL loss and those without (p < 0.05), while no difference could be found in SAP. The AUCs of MD followed a similar pattern, with FDF and FDT matrix perimetry having a suitable AUC of >0.6. AUCs of PSD were not reliable in all of the three VF devices.
Conclusions
The sensitivity for detection of RNFL loss in early glaucoma seems to be higher in FDF and FDT matrix than SAP perimetry, while specifity was highest in SAP. Thus, simultaneous performance of FDF/FDT matrix and SAP perimetry seems beneficial for the correct diagnosis of early glaucoma in patients.




Similar content being viewed by others

References
Quigley HA (1996) Number of people with glaucoma worldwide. Br J Ophthalmol 80:389–393
Clement CI, Goldberg I, Healey PR, Graham S (2009) Humphrey matrix frequency doubling perimetry for detection of visual-field defects in open-angle glaucoma. Br J Ophthalmol 93:582–588
Kim TW, Zangwill LM, Bowd C, Sample PA, Shah N, Weinreb RN (2007) Retinal nerve fiber layer damage as assessed by optical coherence tomography in eyes with a visual field defect detected by frequency doubling technology perimetry but not by standard automated perimetry. Ophthalmology 114:1053–1057
Harwerth RS, Carter-Dawson L, Shen F, Smith EL 3rd, Crawford ML (1999) Ganglion cell losses underlying visual field defects from experimental glaucoma. Invest Ophthalmol Vis Sci 40:2242–2250
Johnson CA (1995) The Glenn A. Fry Award lecture. Early losses of visual function in glaucoma. Optom Vis Sci 72:359–370
Kondo Y, Yamamoto T, Sato Y, Matsubara M, Kitazawa Y (1998) A frequency-doubling perimetric study in normal-tension glaucoma with hemifield defect. J Glaucoma 7:261–265
Medeiros FA, Sample PA, Weinreb RN (2004) Frequency doubling technology perimetry abnormalities as predictors of glaucomatous visual field loss. Am J Ophthalmol 137:863–871
Martin PR, White AJ, Goodchild AK, Wilder HD, Sefton AE (1997) Evidence that blue-on cells are part of the third geniculocortical pathway in primates. Eur J Neurosci 9:1536–1541
Johnson CA (1994) Selective versus nonselective losses in glaucoma. J Glaucoma 1:32–44
White AJ, Sun H, Swanson WH, Lee BB (2002) An examination of physiological mechanisms underlying the frequency-doubling illusion. Invest Ophthalmol Vis Sci 43:3590–3599
Sample PA, Bosworth CF, Blumenthal EZ, Girkin C, Weinreb RN (2000) Visual function-specific perimetry for indirect comparison of different ganglion cell populations in glaucoma. Invest Ophthalmol Vis Sci 41:1783–1790
Spry PG, Johnson CA, McKendrick AM, Turpin A (2001) Variability components of standard automated perimetry and frequency-doubling technology perimetry. Invest Ophthalmol Vis Sci 42:1404–1410
Lamparter J, Aliyeva S, Schulze A, Berres M, Pfeiffer N, Hoffmann EM (2013) Standard automated perimetry versus matrix frequency doubling technology perimetry in subjects with ocular hypertension and healthy control subjects. PLoS One 8:e57663
Lamparter J, Russell RA, Schulze A, Schuff AC, Pfeiffer N, Hoffmann EM (2012) Structure–function relationship between FDF, FDT, SAP, and scanning laser ophthalmoscopy in glaucoma patients. Invest Ophthalmol Vis Sci 53:7553–7559
Spry PG, Johnson CA, Mansberger SL, Cioffi GA (2005) Psychophysical investigation of ganglion cell loss in early glaucoma. J Glaucoma 14:11–19
Sample PA, Medeiros FA, Racette L et al (2006) Identifying glaucomatous vision loss with visual-function-specific perimetry in the diagnostic innovations in glaucoma study. Invest Ophthalmol Vis Sci 47:3381–3389
Mulak M, Szumny D, Sieja-Bujewska A, Kubrak M (2012) Heidelberg Edge Perimeter employment in glaucoma diagnosis–preliminary report. Adv Clin Exp Med 21:665–670
Racette L, Medeiros FA, Zangwill LM, Ng D, Weinreb RN, Sample PA (2008) Diagnostic accuracy of the matrix 24–2 and original N-30 frequency-doubling technology tests compared with standard automated perimetry. Invest Ophthalmol Vis Sci 49:954–960
Burgansky-Eliash Z, Wollstein G, Patel A et al (2007) Glaucoma detection with matrix and standard achromatic perimetry. Br J Ophthalmol 91:933–938
Liu S, Lam S, Weinreb RN et al (2011) Comparison of standard automated perimetry, frequency-doubling technology perimetry, and short-wavelength automated perimetry for detection of glaucoma. Invest Ophthalmol Vis Sci 52:7325–7331
Hasler S, Sturmer J (2012) First experience with the Heidelberg Edge Perimeter on patients with ocular hypertension and preperimetric glaucoma. Klin Monatsbl Augenheilkd 229:319–322
Pinto LM, Costa EF, Melo LA Jr et al (2014) Structure–function correlations in glaucoma using matrix and standard automated perimetry versus time-domain and spectral-domain OCT devices. Invest Ophthalmol Vis Sci 55:3074–3080
Cellini M, Toschi PG, Strobbe E, Balducci N, Campos EC (2012) Frequency doubling technology, optical coherence technology and pattern electroretinogram in ocular hypertension. BMC Ophthalmol 1:12–33
Reus NJ, Lemij HG, Garway-Heath DF et al (2010) Clinical assessment of stereoscopic optic disc photographs for glaucoma: The European Optic Disc Assessment Trial. Ophthalmology 117:717–723
Jampel HD, Friedman D, Quigley H et al (2009) Agreement among glaucoma specialists in assessing progressive disc changes from photographs in open-angle glaucoma patients. Am J Ophthalmol 147:39–44.e1
Townsend KA, Wollstein G, Schuman JS (2009) Imaging of the retinal nerve fibre layer for glaucoma. Br J Ophthalmol 93:139–143
Leung CK, Lam S, Weinreb RN et al (2010) Retinal nerve fiber layer imaging with spectral-domain optical coherence tomography: analysis of the retinal nerve fiber layer map for glaucoma detection. Ophthalmology 117:1684–1691
Hood DC, Anderson SC, Wall M, Raza AS, Kardon RH (2009) A test of a linear model of glaucomatous structure-function loss reveals sources of variability in retinal nerve fiber and visual field measurements. Invest Ophthalmol Vis Sci 50:4254–4266
Hood DC, Fortune B, Arthur SN et al (2008) Blood vessel contributions to retinal nerve fiber layer thickness profiles measured with optical coherence tomography. J Glaucoma 17:519–528
Acknowledgments
The authors thank the Dean of the Medical Faculty of Muenster for supporting their work. Furthermore, we thank Heidelberg Engineering for providing the HeidelbergEdge Perimeter.
Conflict of interest
The HEP perimeter was given as a donation from Heidelberg Engineering for the time span of the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Prokosch, V., Eter, N. Correlation between early retinal nerve fiber layer loss and visual field loss determined by three different perimetric strategies: white-on-white, frequency-doubling, or flicker-defined form perimetry. Graefes Arch Clin Exp Ophthalmol 252, 1599–1606 (2014). https://doi.org/10.1007/s00417-014-2718-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-014-2718-z