
Abstract
Background
Persistent vertical diplopia may occur after cataract surgery as a rare complication of retro- or parabulbar anesthesia. This is probably caused by structural changes in the muscles, altering muscular elasticity and function and thus complicating setting of the dosage for corrective strabismus surgery. The aim of our study was to investigate the effect of strabismus surgery in this specific motility disorder.
Methods
The findings from 15 consecutive patients (six women, nine men, median age 76 years), who had undergone initial strabismus surgery in our eye clinic between 2007 and 2010 due to vertical diplopia following cataract surgery, were investigated retrospectively. In all cases, cataract surgery had been performed under retro- or parabulbar anesthesia.
Results
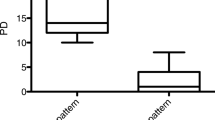
Preoperatively, all affected eyes (five right eyes, ten left eyes) showed hypotropia with elevation deficiency and overaction of the inferior rectus muscle and/or superior oblique muscle on down-gaze. The median vertical deviation in primary position was 9.1 deg (min. 4.6, max. 24.7), measured with the alternate prism cover test, and 8 deg (min. 3.5, max.18) at the tangent screen of Harms. In all cases, the inferior rectus muscle was recessed 3 to 6 mm (median 3.5 mm). On the first day after surgery, the median angle of squint in primary position was 2.3 deg (min. 0, max. 10.2), when measured with the alternate prism cover test, with a mean dose–effect relationship of 1.8 ± 0.7 deg angle reduction per millimetre recession (median 1.9 deg/mm). In the postoperative period, eight patients examined after 2 to 20 months (median 3.5 months) showed a median vertical deviation of 5.7 deg (min. 1.7, max. 11.3), with a mean dose–effect relationship of 1.7 ± 1.3 deg/mm (median 1.8 deg/mm), but the values ranged widely. Four patients were not examined but interviewed by telephone. There was no feed-back from three patients. Six of 12 follow-up patients had no complaints, three had prisms to correct a persisting angle, and three patients needed further squint surgery.
Conclusions
The efficacy of inferior rectus muscle recession for correction of hypotropia following cataract surgery with local anesthesia ranged widely. In this condition, operating on one muscle is a good option for correction of squint angles of less than 12 deg. Squint angle enlargement can occur in the postoperative course, and may necessitate further surgery.



Similar content being viewed by others


References
Yangüela J, Gomez-Arnau JI, Martin-Rodrigo JC, Andueza A, Gili P, Paredes B, Porras MC, González del Valle F, Arias A (2004) Diplopia after cataract surgery: comparative results after topical or regional injection anesthesia. Ophthalmology 111:686–692
Johnson DA (2001) Persistent vertical binocular diplopia after cataract surgery. Am J Ophthalmol 132:831–835
Nayak H, Kersey JP, Oystreck DT, Cline RA, Lyons CJ (2008) Diplopia following cataract surgery: a review of 150 patients. Eye 22:1057–1064
Rainin EA, Carlson BM (1985) Postoperative diplopia and ptosis. A clinical hypothesis based on myotoxicity of local anaesthetics. Arch Ophthalmol 103:1337–1339
Carlson BM, Emerick S, Komorowski TE, Rainin EA, Shepard BM (1992) Extraocular muscle regeneration in primates. Local anesthetic-induced lesions. Ophthalmology 99:582–589
Neugebauer A, Fricke J, Pink U, Rüssmann W (2000) Vertical and cyclotorsional deviations following peribulbar anesthesia. Graefes Arch Clin Exp Ophthalmol 238:119–122
Kim JH, Hwang JM (2006) Imaging of the superior rectus in superior rectus overaction after retrobulbar anesthesia. Ophthalmology 113:1681–1684
Hamed LM, Mancuso A (1991) Inferior rectus muscle contracture syndrome after retrobulbar anesthesia. Ophthalmology 98:1506–1512
Hamilton SM, Elsas FJ, Dawson TL (1993) A cluster of patients with inferior rectus restriction following local anesthesia for cataract surgery. J Pediatr Ophthalmol Strabismus 30:288–291
Costa PG, Debert I, Passos LB, Polati M (2006) Persistent diplopia and strabismus after cataract surgery under local anesthesia. Binocul Vis Strabismus Q 21:155–158
Pearce IA, McCready PM, Watson MP, Taylor RH (2000) Vertical diplopia following local anaesthetic cataract surgery: predominantly a left eye problem? Eye 14:180–184
Capó H, Roth E, Johnson T, Muñoz M, Siatkowski RM (1996) Vertical strabismus after cataract surgery. Ophthalmology 103:918–921
Capó H, Guyton DL (1996) Ipsilateral hypertropia after cataract surgery. Ophthalmology 103:721–744
Zeiss C, Goersch H (2000) Handbuch für Augenoptik. C.Maurer, Geislingen/Steige
Rüssmann W, Neugebauer A, Fricke J (2006) Praktische Augenmuskelchirurgie. Kaden, Heidelberg
Eckstein A, Weiermüller C, Holdt M, Esser J (2011) Schielformen und Augenmuskeloperationen nach Orbitadekompression. Z prakt Augenheilk 32:335–344
Esser J, Schittkowski M, Eckstein A (2011) Graves' orbitopathy: inferior rectus tendon elongation for large vertical squint angles that cannot be corrected by simple muscle recession. Klin Monatsbl Augenheilkd 228:880–886
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schild, A.M., Fricke, J. & Neugebauer, A. Inferior rectus muscle recession as a treatment for vertical diplopia following cataract extraction. Graefes Arch Clin Exp Ophthalmol 251, 189–194 (2013). https://doi.org/10.1007/s00417-012-1996-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-012-1996-6