
Abstract
Background
Disease and treatment-associated immune system abnormalities may confer higher risk of Coronavirus disease 2019 (COVID-19) to people with multiple sclerosis (PwMS). We assessed modifiable risk factors associated with COVID-19 in PwMS.
Methods
Among patients referring to our MS Center, we retrospectively collected epidemiological, clinical and laboratory data of PwMS with confirmed COVID-19 between March 2020 and March 2021 (MS-COVID, n = 149). We pursued a 1:2 matching of a control group by collecting data of PwMS without history of previous COVID-19 (MS-NCOVID, n = 292). MS-COVID and MS-NCOVID were matched for age, expanded disability status scale (EDSS) and line of treatment. We compared neurological examination, premorbid vitamin D levels, anthropometric variables, life-style habits, working activity, and living environment between the two groups. Logistic regression and Bayesian network analyses were used to evaluate the association with COVID-19.
Results
MS-COVID and MS-NCOVID were similar in terms of age, sex, disease duration, EDSS, clinical phenotype and treatment. At multiple logistic regression, higher levels of vitamin D (OR 0.93, p < 0.0001) and active smoking status (OR 0.27, p < 0.0001) emerged as protective factors against COVID-19. In contrast, higher number of cohabitants (OR 1.26, p = 0.02) and works requiring direct external contact (OR 2.61, p = 0.0002) or in the healthcare sector (OR 3.73, p = 0.0019) resulted risk factors for COVID-19. Bayesian network analysis showed that patients working in the healthcare sector, and therefore exposed to increased risk of COVID-19, were usually non-smokers, possibly explaining the protective association between active smoking and COVID-19.
Conclusions
Higher Vitamin D levels and teleworking may prevent unnecessary risk of infection in PwMS.
Similar content being viewed by others


Background
Demographic, ecological, and politico-economic factors together with comorbidities have influenced the severity of Coronavirus disease 2019 (COVID-19) worldwide [1]. Among others, this pandemic has also raised health concerns related to people with multiple sclerosis (PwMS) in the acute phase of the outbreak. These people have been considered at higher risk to contract SARS-CoV-2 infection and have a more severe COVID-19 course due to their clinical disability, comorbidities, disease-associated immune alterations and the use of disease modifying therapies (DMTs) [2, 3].
In the general population more than 6,500,000 deaths have been reported in the world [4]. Data collected during the pandemic suggest that COVID-19 may determine acute detrimental immunologic, metabolic, and thromboembolic abnormalities. Furthermore, long-term persistence of neurologic and neuropsychiatric manifestations was also described in COVID-19 survivors [5] and was associated with pro-inflammatory unbalance [6], suggesting that such immunologic changes may persist long after the resolution of the infection.
Iaffaldano et al. [7] have recently observed that in PwMS presence of comorbidities, female sex and younger age may increase the risk to develop a COVID infection by approximately 70%, 25% and 10% respectively. Furthermore, PwMS who developed COVID-19 were more frequently treated during the course of the disease with high efficacy DMT or moderate efficacy DMTs followed by high efficacy DMT strategies (18.23% vs 15.60%, 30.17% vs 23.11%).
Among PwMS, older age, male sex, concomitant comorbidities, higher disability, ongoing anti CD-20 therapy and recent methylprednisolone administration were associated with a worse prognosis [3, 8,9,10,11]. These findings are in line with those obtained from large-scale cohorts in Western Countries which suggest that in the general population risk factors for severe COVID-19 disease course are older age, male sex, and concomitant comorbidities [12, 13]. The definition of such demographic and clinical features are helpful for the identification of those patients at high-risk of severe COVID-19, but still their utility is limited in terms of preventive interventions as they are non-modifiable traits. In contrast, studies on the general population have highlighted that also modifiable factors such as higher body mass index (BMI), higher glycated hemoglobin and smoking [14], are associated with a worse outcome, opening the way to tailored preventive strategies.
So far, no study has tried to identify lifestyle and other modifiable variables associated with an increased risk of contracting SARS-CoV-2 infection in PwMS. Therefore, in this case–control study we focused on the identification of anthropometric features, life-style habits, working activities and living environment conditions associated with COVID-19 in PwMS. Clinical data including pre-morbid disability, treatment, and comorbidities were also evaluated.
Methods
Study population, study setting, and data collection
We enrolled patients afferent to the Multiple Sclerosis Center of the IRCCS San Raffaele Hospital, who had a diagnosis of MS according to 2017 McDonald Criteria [15]. Data were retrospectively collected in PwMS who had a confirmed COVID-19 infection between March 2020 and March 2021 (MS-COVID). Inclusion criteria were: (i) typical clinical manifestations of COVID-19, such as fever, cough and dyspnea [16], plus (ii) having a positive Nucleic Acid Amplification Test (NAAT) for SARS-CoV-2 at the time of the symptoms or a positive IgG or IgM SARS-CoV-2 serology within the three months following typical COVID-19 symptoms. Data collection was obtained by direct patient interview within the first year after infection.
At the same time, we randomly selected a group of PwMS without a history of symptoms suggestive of COVID-19 infection and without COVID-19 diagnosis between March 2020 and March 2021 (MS-NCOVID). MS-COVID and MS-NCOVID patients were 1:2 matched by age (± 4 years), sex, expanded disability status scale (EDSS, ± 0.5), disease duration (± 3 years), and line of treatment (first or second line). First line treatments were glatiramer acetate, interferon, teriflunomide, dimethyl fumarate, and azathioprine, while second line treatment were fingolimod, natalizumab, cladribile, rituximab, ocrelizumab or alemtuzumab. As per historical moment, all participants were not vaccinated against SARS-CoV-2.
Demographic, anthropometric, clinical, laboratory, and life-style features
In both groups, we retrospectively collected demographic and anthropometric features, clinical data, laboratory tests, working activity, living condition, and life-style habits.
Demographic variables were age and sex, while anthropometric variables were height, weight, and BMI. Clinical variables included: Expanded Disability Status Scale (EDSS) [17], MS clinical phenotype (relapsing–remitting [RR], primary progressive [PP], secondary progressive [SP]), disease duration, time from MS diagnosis, number of comorbidities and ongoing treatment with DMTs and, if so, administration of first- or second-line therapies. Laboratory tests were performed in the six months before COVID-19, according to the routine monitoring of these patients for DMT, or before data collection for MS-NCOVID and included vitamin D levels (ng/ml). Classes of working activities were: (1) no external contacts (unemployed, telework or working alone on workplace), (2) work requiring direct external contact (with colleagues or public), (3) health-care work. Living conditions were assessed by the evaluation of number of cohabitants, presence and number of school-aged children. Life-style behaviours such as smoke (never smoker, previous smoker, current smoker) were also collected.
Statistical analysis
For all statistical analyses, the significant level was 0.05. All statistical analyses were performed using R 3.5.0 (http://www.R-project.org/).
Between-group comparison of demographic, anthropometric, clinical, laboratory, and life-style features
Continuous variables were reported as median and interquartile range, while categorical variables as absolute and relative frequencies. Disease duration was computed at COVID-19 onset for the MS-COVID group and at the time of the interview for the MS-NCOVID group. Single DMTs in the two groups were reported only descriptively.
Logistic regression analysis for predicting MS-COVID vs MS-NCOVID status
Univariate and multiple logistic regression analyses were employed to evaluate the association between patients’ features and SARS-CoV-2 infection. The features resulting matched between the MS-COVID and MS-NCOVID groups were not included in the analysis. In the univariate analysis, p-values were adjusted with Bonferroni’s correction to account for multiple testing. In the multiple regression analysis, the final model was obtained with a backward procedure of variable selection.
Post-hoc Bayesian network and association analysis
A Bayesian Network model was estimated considering the same features evaluated in the logistic regression analysis, to explore how variables are associated with COVID-19 infection accounting for their complex relationships. Since this analysis required the usage of only categorical variables, numerical variables were categorized either with clinical cut-off or quartiles (number of comorbidities: 0, 1, ≥ 2; Number of cohabitants: 0, 1, 2, ≥ 3; BMI: underweight, normal, overweight; Vitamin D levels: < 23, ≥ 23 and < 31, ≥ 31 and < 39, ≥ 39). The BN was estimated using the Tabu greedy search (TABU) algorithm with Akaike information criterion (AIC) score function. For variables resulting associated with COVID-19 infection, we explored the association with other patients’ features with Fisher’s exact test or Mann–Whitney U test.
Results
Between-group comparison of matched features in MS-COVID and MS-NCOVID patients
As expected, MS-COVID and MS-NCOVID patients were similar in terms of a priori matched variables, specifically: age, sex distribution, disease duration, EDSS, disease phenotype and line of DMTs (Table 1). MS-COVID and MS-NCOVID patients were mainly female (66% and 65% respectively), and the median age was of 41 and 45 years. The median disease duration was relatively long in both groups (10 and 12 years) and disability was usually mild (median EDSS 1.5 and 2.0). The majority of patients had a relapsing–remitting disease (95% in both groups) and were treated with first-line DMTs (56–52%). Detailed specifics of ongoing DMT are summarized in Table 2.
Associations between risk factors and SARS-CoV-2 infection
Table 3 reports the descriptive statistics of anthropometric features, laboratory variables, working activities, living conditions and life-style habits in the two groups. At univariate logistic regression analysis (Table 3), higher vitamin D levels resulted protective for COVID-19 disease (odds ratio [OR]; 95% confidence interval, [CI]: 0.94 [0.91;0.95], adjusted p value < 0.0001). In contrast, the number of cohabitants (OR [95% CI]: 1.36 [1.53;1.61], adjusted p value = 0.004) and the working activity during the pandemic (jobs with direct external contact: OR [95% CI]: 2.34 [1.53;3.61], adjusted p-value = 0.0009; healthcare jobs: OR [95% CI]: 3.55 [1.75;7.27], adjusted p value = 0.0040) resulted risk factors for SARS-CoV-2 infection.
Smoking status emerged as protective against SARS-CoV-2 infection (OR [95% CI] = 0.33 [0.19;0.56], adjusted p value = 0.0004).
The final multiple logistic regression model confirmed the results of the univariate logistic regression analysis, as reported in Table 4.
Bayesian network and association analysis
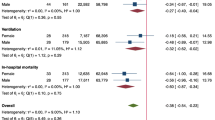
Given the protective association between active smoking and COVID-19 disclosed by the logistic regression analysis, we estimated a Bayesian Network (BN) model to assess possible complex relationships among the variables analysed, considering the same features evaluated in the logistic regression analysis. Specifically, we found in the BN that a specific working activity was also associated with smoking status, and by a further association analysis this resulted significant (adjusted p = 0.010), as healthcare professionals were usually non-smokers. The BN is shown in Fig. 1, while results of between-group comparisons of non-smokers during the pandemic (i.e., both never smokers and previous smokers) and active smokers are reported in Table 5.

Bayesian Network analysis for exploring the dependence structure among the variables and SARS-CoV-2 infection. Numerical variables were categorized as described in the Statistical methods
Discussion
This is a single-center case–control study aimed to evaluate modifiable risk factors for SARS-CoV-2 infection in PwMS. Comorbidities were also included in the analysis to avoid their nuisance effects in the interpretation of data. In our analysis, at multiple logistic regression, higher levels of vitamin D (OR 0.93, p < 0.0001) emerged as protective factors against SARS-CoV-2 infection. In contrast, higher number of cohabitants (OR 1.26, p = 0.02) and works requiring direct external contact (OR 2.61, p = 0.0002) or in the healthcare sector (OR 3.73, p = 0.0019) resulted risk factors for COVID-19 disease. In addition to higher vitamin D levels, also active smoking status (OR 0.27, p < 0.0001) emerged as protective factors against SARS-CoV-2 infection.
In the general population, other studies found that people with 25OHD levels ≥ 30 ng/ml had lower risk of SARS-CoV2 infection, lower risk of severe COVID-19 and lower COVID-19 mortality than 25OHD-deficient patients [18,19,20]. Vitamin D exerts immunoregulatory properties on both innate and adaptive immune systems. Its deficit is associated with increased autoimmunity as well as an increased susceptibility to infection [21], possibly explaining why lower vitamin D levels confer a higher risk of SARS-CoV-2 infection even in the general population. Moreover, there is established evidence that vitamin D deficiency is relevant for MS pathogenesis, since it was consistently found as a significant risk factor for the development of the disease [22]. More recently, low levels of vitamin D were also reported as a negative prognostic factor in patients with MS, given their association with more severe MRI activity, cognitive impairment and evolution to secondary progressive disease course [22,23,24]. These observations strengthen the indication of maintaining 25(OH)D levels among PwMS of at least 30 ng/ml (75 nmol/L), and preferably 40–60 ng/mL (100–150 nmol/L) [25], especially during the ongoing pandemic.
Other studies showed that housing conditions, such as overcrowded housing, are an important risk factor for SARS-CoV-2 infection [1, 26]. Household exposure can be a relevant risk factor for SARS-CoV-2 infection in patients who rarely leave their home. In line with this, a study demonstrated that the odd for COVID-19 seropositivity among cancer patients was related to intrafamiliar exposure [27]. To the best of our knowledge, no other study demonstrated that specifically the number of cohabitants also increases the risk in PwMS. This result is particularly challenging if we consider that reduced human interaction related to COVID-19 has a profound impact on organic and mental health [1, 26, 27]. Although it is associated with an increased risk of COVID-19 infection, we still encourage social interactions between PwMS and their relatives, but we recommend strict adherence to COVID-19 preventive measures, such as FFP2 mask wearing and frequent hand sanitizing.
A working activity requiring a direct contact with people outside the family (i.e., colleagues or public, healthcare jobs) resulted a risk factor for COVID-19 disease. In line with this hypothesis, distant working was largely adopted, especially during the first phase of the pandemic. However, many employers are now reducing distant work opportunities. Our results suggest that this policies could be harmful for PwMS, where we should encourage teleworking whenever possible. This is of increasing importance because of the ongoing energetic crisis, as patients may favour public to private transportation, with the former associated with increased COVID-19 [28].
Unexpectedly, we found that active smoking status was associated with a reduced risk of developing COVID-19. Smoking is associated with increased severity of COVID-19 infection in the general population [29,30,31,32,33], but initial studies found it to be negatively associated with the risk of developing COVID-19 in the general population [34,35,36]. Subsequent studies demonstrated that smoking is positively associated with the risk of developing COVID-19 in the general population [29, 31, 32]. Although a consistent answer to this “smoking paradox” is hard to extract from the literature, the protective effect of smoking was hardly criticised [37]. To assess whether other features associated with smoking can explain such a risk reduction in our sample, we applied a Bayesian Network analysis which found an association between non-smoking status and working in the healthcare sector, which was, as expected [38], strongly associated in the multiple logistic regression with the risk of SARS-CoV-2 infection (OR [95% CI]: 3.73 [1.64;8.70]). Another possible explanation is that smokers may have chronic mild respiratory symptoms, leading to an underestimation of possible COVID-19 related symptoms and therefore a lower rate of COVID-19 diagnosis. Further studies are clearly needed to clarify the association between smoking and COVID-19. Nevertheless, we strongly discourage smoking among PwMS considering its detrimental effect on disease progression, disease activity, atrophy and disability [39].
This study is not without limitations. First, data collection was retrospective. However, data for this study were collected through a direct patients-neurologist’s interview and not only though medical records, which should have increased the accuracy of the information collected. Another limitation is the inclusion of patients infected during the first pandemic wave, but this had the advantage of avoiding the confounding effect of vaccination, which we know may have a different efficacy according to patients’ treatment [40]. Furthermore our study population had relatively mild clinical disability (reflecting our centre’s population). Further studies are needed to establish whether these findings are applicable to patients with more severe levels of clinical disability.
Although MS-NCOVID patients had no history of symptoms suggestive of COVID-19 infection and no COVID-19 diagnosis between March 2020 and March 2021, they were not necessarily tested negative for COVID-19 serological status. Therefore it is possible that some patients may have developed asymptomatic COVID-19 and have been misallocated in the MS-NCOVID group.
Even though patients were matched for line of treatment, the frequency of ongoing anti CD-20 therapy was higher in MS-COVID group (Table 2). Anti CD-20 therapies are associated with more severe COVID-19 [2, 3], but were not identified as specific non-modifiable risk factor for COVID-19 [7].
In conclusion, our study demonstrated that several modifiable factors can favour or contrast SARS-CoV-2 infection in PwMS, and may help clinicians to protect those patients with a priori risk factors of severe COVID-19 severity. Pursuing an educational policy towards employers aimed at emphasizing the community and social importance of telework as well as the maintenance of protective personal measures and behaviours on public transportation and outdoor places may prevent unnecessarily risk of infection in these patients. Moreover, this study reinforces the importance of careful monitoring and supplementation of vitamin D levels in PwMS.
Data availability
The anonymized dataset used and analysed during the current study is available from the corresponding author upon reasonable request.
References
Varshney K, Glodjo T, Adalbert J (2022) Overcrowded housing increases risk for COVID-19 mortality: an ecological study. BMC Res Notes 15(1):126
Perez CA, Zhang GQ, Li X, Huang Y, Lincoln JA, Samudralwar RD et al (2021) COVID-19 severity and outcome in multiple sclerosis: results of a national, registry-based, matched cohort study. Mult Scler Relat Disord 55:103217
Sormani MP, Schiavetti I, Carmisciano L, Cordioli C, Filippi M, Radaelli M, et al. (2022) COVID-19 severity in multiple sclerosis: putting data into context. Neurol Neuroimmunol Neuroinflamm 9(1):e1105
https://covid19.who.int/ [Available from: https://covid19.who.int/.
Desai AD, Lavelle M, Boursiquot BC, Wan EY (2022) Long-term complications of COVID-19. Am J Physiol Cell Physiol 322(1):C1–C11
Group P-CC (2022) Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalisation in the UK: a prospective observational study. Lancet Respir Med 10(8):761–75.
Iaffaldano P, Lucisano G, Manni A, Paolicelli D, Patti F, Capobianco M et al (2022) Risk of getting COVID-19 in people with multiple sclerosis: a case-control study. Neurol Neuroimmunol Neuroinflamm 9(2):e1141
Louapre C, Collongues N, Stankoff B, Giannesini C, Papeix C, Bensa C et al (2020) Clinical characteristics and outcomes in patients with coronavirus disease 2019 and multiple sclerosis. JAMA Neurol 77(9):1079–1088
Salter A, Fox RJ, Newsome SD, Halper J, Li DKB, Kanellis P et al (2021) Outcomes and risk factors associated with SARS-CoV-2 infection in a North American registry of patients with multiple sclerosis. JAMA Neurol 78(6):699–708
Sormani MP, De Rossi N, Schiavetti I, Carmisciano L, Cordioli C, Moiola L et al (2021) Disease-modifying therapies and coronavirus disease 2019 severity in multiple sclerosis. Ann Neurol 89(4):780–789
Sormani MP, Salvetti M, Labauge P, Schiavetti I, Zephir H, Carmisciano L et al (2021) DMTs and Covid-19 severity in MS: a pooled analysis from Italy and France. Ann Clin Transl Neurol 8(8):1738–1744
Booth A, Reed AB, Ponzo S, Yassaee A, Aral M, Plans D et al (2021) Population risk factors for severe disease and mortality in COVID-19: a global systematic review and meta-analysis. PLoS One 16(3):e0247461
Kaeuffer C, Le Hyaric C, Fabacher T, Mootien J, Dervieux B, Ruch Y, et al. (2020) Clinical characteristics and risk factors associated with severe COVID-19: prospective analysis of 1045 hospitalised cases in North-Eastern France, March 2020. Euro Surveill 25(48)
Ho FK, Celis-Morales CA, Gray SR, Katikireddi SV, Niedzwiedz CL, Hastie C et al (2020) Modifiable and non-modifiable risk factors for COVID-19, and comparison to risk factors for influenza and pneumonia: results from a UK Biobank prospective cohort study. BMJ Open 10(11):e040402
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G et al (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17(2):162–173
da Rosa Mesquita R, Francelino Silva Junior LC, Santos Santana FM, Farias de Oliveira T, Campos Alcantara R, Monteiro Arnozo G, et al. (2021) Clinical manifestations of COVID-19 in the general population: systematic review. Wien Klin Wochenschr 133(7–8):377–82.
Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33(11):1444–1452
Oristrell J, Oliva JC, Casado E, Subirana I, Dominguez D, Toloba A et al (2022) Vitamin D supplementation and COVID-19 risk: a population-based, cohort study. J Endocrinol Invest 45(1):167–179
Barrea L, Verde L, Grant WB, Frias-Toral E, Sarno G, Vetrani C et al (2022) Vitamin D: a role also in long COVID-19? Nutrients 14(8):1625
Karonova TL, Chernikova AT, Golovatyuk KA, Bykova ES, Grant WB, Kalinina OV et al (2022) Vitamin D Intake may reduce SARS-CoV-2 infection morbidity in health care workers. Nutrients 14(3):505
Aranow C (2011) Vitamin D and the immune system. J Investig Med 59(6):881–886
Sintzel MB, Rametta M, Reder AT (2018) Vitamin D and multiple sclerosis: a comprehensive review. Neurol Ther 7(1):59–85
Mowry EM, Waubant E, McCulloch CE, Okuda DT, Evangelista AA, Lincoln RR et al (2012) Vitamin D status predicts new brain magnetic resonance imaging activity in multiple sclerosis. Ann Neurol 72(2):234–240
Cortese M, Munger KL, Martinez-Lapiscina EH, Barro C, Edan G, Freedman MS et al (2020) Vitamin D, smoking, EBV, and long-term cognitive performance in MS: 11-year follow-up of BENEFIT. Neurology 94(18):e1950–e1960
Gandhi F, Jhaveri S, Avanthika C, Singh A, Jain N, Gulraiz A et al (2021) Impact of vitamin D supplementation on multiple sclerosis. Cureus 13(10):e18487
Lim C, Nam Y, Oh WS, Ham S, Kim E, Kim M et al (2022) Characteristics of transmission routes of COVID-19 cluster infections in Gangwon Province. Korea Epidemiol Infect 150:e19
Palka-Kotlowska M, Custodio-Cabello S, Oliveros-Acebes E, Khosravi-Shahi P, Cabezon-Gutierrez L (2021) Review of risk of COVID-19 in cancer patients and their cohabitants. Int J Infect Dis 105:15–20
Ellingjord-Dale M, Kalleberg KT, Istre MS, Nygaard AB, Brunvoll SH, Eggesbo LM et al (2022) The use of public transport and contraction of SARS-CoV-2 in a large prospective cohort in Norway. BMC Infect Dis 22(1):252
Hopkinson NS, Rossi N, El-Sayed Moustafa J, Laverty AA, Quint JK, Freidin M, et al. (2021) Current smoking and COVID-19 risk: results from a population symptom app in over 2.4 million people. Thorax 76(7):714–22.
Umnuaypornlert A, Kanchanasurakit S, Lucero-Prisno DEI, Saokaew S (2021) Smoking and risk of negative outcomes among COVID-19 patients: a systematic review and meta-analysis. Tob Induc Dis 19:09
He Y, Sun J, Ding X, Wang Q (2021) Mechanisms in which smoking increases the risk of COVID-19 infection: a narrative review. Iran J Public Health 50(3):431–437
Haddad C, Bou Malhab S, Sacre H, Salameh P (2021) Smoking and COVID-19: a scoping review. Tob Use Insights 14:1179173X21994612.
Patanavanich R, Glantz SA (2021) Smoking is associated with worse outcomes of COVID-19 particularly among younger adults: a systematic review and meta-analysis. BMC Public Health 21(1):1554
Usman MS, Siddiqi TJ, Khan MS, Patel UK, Shahid I, Ahmed J et al (2021) Is there a smoker’s paradox in COVID-19? BMJ Evid Based Med 26(6):279–284
Paleiron N, Mayet A, Marbac V, Perisse A, Barazzutti H, Brocq FX et al (2021) Impact of tobacco smoking on the risk of COVID-19: a large scale retrospective cohort study. Nicotine Tob Res 23(8):1398–1404
Wenzl T (2020) Smoking and COVID-19 A review of studies suggesting a protective effect of smoking against COVID-19. Pubblication office of the European Union
van Westen-Lagerweij NA, Meijer E, Meeuwsen EG, Chavannes NH, Willemsen MC, Croes EA (2021) Are smokers protected against SARS-CoV-2 infection (COVID-19)? The origins of the myth. NPJ Prim Care Respir Med 31(1):10
Gholami M, Fawad I, Shadan S, Rowaiee R, Ghanem H, Hassan Khamis A et al (2021) COVID-19 and healthcare workers: a systematic review and meta-analysis. Int J Infect Dis 104:335–346
Lie IA, Wesnes K, Kvistad SS, Brouwer I, Wergeland S, Holmoy T et al (2022) The effect of smoking on long-term gray matter atrophy and clinical disability in patients with relapsing-remitting multiple sclerosis. Neurol Neuroimmunol Neuroinflamm 9(5):e200008
Sormani MP, Inglese M, Schiavetti I, Carmisciano L, Laroni A, Lapucci C et al (2021) Effect of SARS-CoV-2 mRNA vaccination in MS patients treated with disease modifying therapies. EBioMedicine 72:103581
Funding
This study has been partially Supported by FISM—Fondazione Italiana Sclerosi Multipla—cod. 2021/C19-R-Single/005 and financed or cofinanced with the '5 per mille' public funding.
Author information
Authors and Affiliations
Contributions
Concept and design: MR, MF. Acquisition, analysis, or interpretation of data: MN, RZ, MC, ER, MF. Drafting of the manuscript: MR, CR, MF. Statistical analysis: RC. Supervision: RMF.
Corresponding author
Ethics declarations
Conflict of interest
Federico Montini has no potential conflicts of interest and reports no disclosures; Agostino Nozzolillo has no potential conflicts of interest and reports no disclosures; Paola M.V. Rancoita has no potential conflicts of interest and reports no disclosures; Chiara Zanetta has no potential conflicts of interest and reports no disclosures; Lucia Moiola received compensation for speaking activities, and/or consulting services from Merck, Biogen, Novartis, Roche, Sanofi, and TEVA; Federica Cugnata has no potential conflicts of interest and reports no disclosures; Federica Esposito received consulting and speaking fees from Novartis, Sanofi Genzyme; Maria A. Rocca received consulting fees from Biogen, Bristol Myers Squibb, Eli Lilly, Janssen, Roche; and speaker honoraria from AstraZaneca, Biogen, Bristol Myers Squibb, Bromatech, Celgene, Genzyme, Horizon Therapeutics Italy, Merck Serono SpA, Novartis, Roche, Sanofi and Teva. She receives research support from the MS Society of Canada, the Italian Ministry of Health, and Fondazione Italiana Sclerosi Multipla. She is Associate Editor for Multiple Sclerosis and Related Disorders; Vittorio Martinelli received compensation for speaking and/or for consultancy and support for travel expenses and participation in Congresses from Biogen, Merck-Serono, Novartis, Genzyme and Teva Pharmaceutical Industries; Massimo Filippi is Editor-in-Chief of the Journal of Neurology, Associate Editor of Human Brain Mapping, Neurological Sciences, and Radiology; received compensation for consulting services from Alexion, Almirall, Biogen, Merck, Novartis, Roche, Sanofi; speaking activities from Bayer, Biogen, Celgene, Chiesi Italia SpA, Eli Lilly, Genzyme, Janssen, Merck-Serono, Neopharmed Gentili, Novartis, Novo Nordisk, Roche, Sanofi, Takeda, and TEVA; participation in Advisory Boards for Alexion, Biogen, Bristol-Myers Squibb, Merck, Novartis, Roche, Sanofi, Sanofi-Aventis, Sanofi-Genzyme, Takeda; scientific direction of educational events for Biogen, Merck, Roche, Celgene, Bristol-Myers Squibb, Lilly, Novartis, Sanofi-Genzyme; he receives research support from Biogen Idec, Merck-Serono, Novartis, Roche, Italian Ministry of Health, Fondazione Italiana Sclerosi Multipla, and ARiSLA (Fondazione Italiana di Ricerca per la SLA).
Ethical standards
Approval was received from the local ethical standards committee on human experimentation (Ethical committee approval no. 101/INT/2020), and written informed consent was obtained from all participants prior to study enrolment, according to the declaration of Helsinki.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Montini, F., Nozzolillo, A., Rancoita, P.M.V. et al. Modifiable risk factors of COVID-19 in patients with multiple sclerosis: a single-centre case–control study. J Neurol 270, 1835–1842 (2023). https://doi.org/10.1007/s00415-023-11618-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-023-11618-0