
Abstract
Background
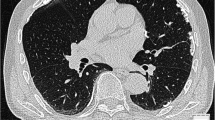
Pulmonary compliance can be viewed as an indicator of distensibility of the lungs, not only in asbestos-induced pulmonary disorders but also in visceral pleural fibrosis extending into the lung parenchyma. In this study we evaluated static compliance measurements in asbestos-derived diseases, especially in patients with parietal pleura plaques. Lung function analyses, especially static lung compliance, were correlated with high-resolution computer tomography examinations.
Methods
Sixty-three patients with parietal pleural plaques, 10 with visceral pleural fibrosis, 39 with parenchymal pulmonary asbestosis together with parietal pleural plaques, and 42 with parenchymal pulmonary asbestosis together with visceral pleural fibrosis were enrolled in the study.
Results
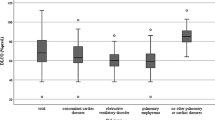
In comparison with patients having only parietal pleural plaques, those having asbestosis and visceral pleural fibrosis showed significant decreases in static lung compliance, diffusing capacity, and vital capacity. Visceral pleural thickening was also associated with significantly reduced FEV1, MEF50, and FEV1/FVC ratios. Multiple regression analyses indicated that the existence of visceral pleural fibrosis (p = 0.017) is the most important factor accounting for a decrease in static compliance. Reference values of static lung compliance differ notably. In comparison with mean reference values, the sensitivity of detecting reduced lung compliance was calculated to be between 9.7 and 45.5 %. Other respiratory function variables failed to show any significant differences.
Conclusion
Our data indicate that the measurement of static compliance is not sufficient for early detection of pulmonary function impairment in patients with parietal pleural plaques.




Similar content being viewed by others

References
Hering KG, Tuengerthal S, Kraus T (2004) Standardisierte CT/HRCT-Klassifikation der Bundesrepublik Deutschland für ar-beits- und umweltbedingte Thoraxerkrankungen. Radiologe 44:500–511
Kusaka Y, Hering KG, Parker JE (2005) International classification of HRCT for occupational and environmental respiratory diseases. Springer, Tokyo
Gevenois PA, De Meartelear V, Madani A et al (1998) Asbestosis, pleural plaques and diffuse pleural thickening: three distinct benign responses to asbestos exposure. Eur Respir J 11:1021–1027
Epler GR, MacLoud T, Gainsler EA et al (1978) Normal chest roentgenograms in chronic diffuse infiltrative disease. N Engl J Med 198:934–949
Hillerdal G, Malmberg P, Hemmingsson A (1990) Asbestos-related lesions of the pleura: parietal plaques compared to diffuse thickening studied with chest roentgenography, computed tomography, lung function, and gas exchange. Am J Ind Med 18:627–639
Brändli O, Leuenberger P, Schindler C et al (2000) Reestimated reference equations for the 5th percentiles of lung function variables in the adult population of Switzerland (SAPALDIA-study). Thorax 55:173–174
Cotes JE, Chinn DJ, Quanjer PH et al (1993) Standardization of the measurement of transfer factor (diffusing capacity). European Community for Steel and Coal. Official statement of the European Respiratory Society. Eur Respir J 6:41–52
Kuster SP, Kuster D, Schindler D et al (2008) Reference equations for lung function screening of healthy never-smoking adults aged 18–80 years. Eur Respir J 31:860–868
van der Lee I, Zanen P, Stigter N et al (2007) Diffusing capacity for nitric oxide: reference values and dependence on alveolar volume. Respir Med 101:1579–1584
MacIntyre N, Crapo RO, Viegi G et al (2005) Standardisation of spirometry. Eur Respir J 26:319–338
Quanjer P, Tammeling GJ, Cotes JE et al (1993) Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests. European Community for Steel and Coal. Official statement of the European Respiratory Society. Eur Respir J 6(suppl):5–40
BK-Report 1/2007 Faserjahre: Berufsgenossenschaftliche Hinweise zur Ermittlung der kumulativen Asbestfaserstaub-Dosis am Arbeitsplatz (Faserjahre) und Bearbeitungshinweise zur Berufskrankheit der gewerblichen Berufsgenossenschaften, Sankt Augustin (1993, 1994, 1997, 2007) [Report Fiber years: BG recommendations to determine the cumulative dose of asbestos dust in the workplace (fiber years) and instructions for the occupational disease]. Hauptverband der gewerblichen Berufsgenossenschaften, Sankt Augustin
Yernault JC, Baran D, Englert M (1977) Effect of growth and aging on the static mechanical lung properties. Bull Eur Physiopathol Respir 13:777–788
Quanjer PH (1983) Standardized lung function testing. Bull Eur Physiopathol Respir 5(Suppl):1–92
Pielesch W, Riedel E, Lüdde E (1984) Calculation of normal values in lung compliance. Respiration 46:69–75
Gillissen A, Schött D, Ulmer WT (1990) Static compliance in probands with healthy lungs and patients with chronic obstructive respiratory tract disease. Pneumologie 44:637–638
Galetke W, Feier C, Muth T et al (2007) Reference values for dynamic and static pulmonary compliance in men. Respir Med 101:1783–1789
Yernault JC, Englert M (1974) Static mechanical lung properties in young adults. Bull Physiopathol Respir (Nancy) 10:435–450
Butler J, White HC, Melville Arnott W (1957) The pulmonary compliance in normal subjects. Clin Sci 16:709–729
Cherniack RM, Hodson A (1963) Compliance of the chest wall in chronic bronchitis and emphysema. J Appl Physiol 18:707–711
Zeilhofer R (1974) Total compliance of lungs and thorax in healthy men (author’s transl)]. Respiration 31:318–331
Zeilhofer R (1966) Respiration mechanic (esophagus pressure method)]. Beitr Klin Erforsch Tuberk Lungenkr 133:278–291
Stead WW, Donald LF, Ebert RV (1952) The elastic properties of the lung in normal men and in patients with chronic pulmonary emphysema. J Lab Clin Med 40:674–681
Gibson GJ, Pride NB (1976) Lung distensibility: the static pressure–volume curve of the lungs and its use in clinical assessment. Br J Dis Chest 70:143–184
Mittmann C, Edelmann NH, Norris AH et al (1965) Relationship between chest wall and pulmonary compliance and age. J Appl Physiol 20:1211–1216
Frank NR, Mead J, Siebens AA et al (1955) Measurements of pulmonary compliance in seventy healthy young adults. J Appl Physiol 9:38–42
Chan CC, Cheong TH, Poh SC et al (1995) Lung elastic recoil in normal young adult Chinese compared with Caucasians. Eur Respir J 8:446–449
Baur X, Wilken D (2010) Effect of asbestos fibre dust exposures on lung function—a systematic review. Pneumologie 64:81–110
Wright PH, Hanson A, Kreel L et al (1980) Respiratory function changes after asbestos pleurisy. Thorax 25:31–36
Valkila EH, Nieminen MM, Moilanen AK et al (1995) Asbestos-induced visceral pleural fibrosis reduces pulmonary compliance. Am J Ind Med 28:363–372
Schwartz DA, Galvin JR, Dayton CS et al (1990) Determinants of restrictive lung function in asbestos-induced pleural fibrosis. J Appl Physiol 68:1932–1937
Zedda S, Aresini G, Chezzi I et al (1973) Lung function in relation to radiographic changes in asbestos workers. Respiration 30:132–140
Bader ME, Bader RA, Teirstein AS et al (1970) Pulmonary function and radiographic changes in 598 workers with varying duration of exposure to asbestos. Mount Sinai J Med 37:492
Gaensler EA, Carrington CB, Coutu RE et al (1972) Pathological, physiological and radiological correlation in the pneumoconiosis. Ann NY Acad Sci 200:574
Acknowledgments
This study was supported by the Deutsche Gesetzliche Unfallversicherung (DGUV) in Sankt Augustin, AZ: FF-FB 131. We thank Prof. Dipl. Ing. Paul Mayer, senior technical inspector of the Berufsgenossenschaft der Keramischen und Glas-Industrie in Würzburg, for calculating the asbestos dose in cumulative fiber-years.
Conflict of interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schneider, J., Arhelger, R., Raab, W. et al. The Validity of Static Lung Compliance in Asbestos-induced Diseases. Lung 190, 441–449 (2012). https://doi.org/10.1007/s00408-012-9388-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-012-9388-6