
Abstract
Study Objectives The poor long-term survival of patients requiring prolonged mechanical ventilation may be due to potentially modifiable factors. We therefore sought to assess the early determinants of long-term survival after discharge from a specialized respiratory unit. Methods Eighty of 113 patients (71%) admitted to a respiratory care unit from June 2001 to August 2003 survived to discharge. Mortality outcomes and dates of death were determined by review of the records and survey in April 2005 of a national Death Master File. Potential determinants of survival after discharge were collected during the admission to the unit. Results Fifty-five percent of patients died within the first year after discharge. Age of 65 years or older, sacral ulcers, a serum creatinine >124 μmol/L, and failure to wean were each individually associated with shorter survival. Age, skin integrity, and wean status on discharge remained independent determinants of survival in a multivariable analysis. In a post-hoc analysis, chronic irreversible neurologic diseases were also independently associated with poor long-term survival. Conclusions Mortality after discharge from a respiratory care unit is high. Interventions that may favorably impact long-term survival in these patients could target the modifiable factors identified, including measures that facilitate weaning and prevent or treat renal dysfunction and skin breakdown.
Similar content being viewed by others

Introduction
About 7% of patients admitted to intensive care units (ICU) require mechanical ventilation for more than 3 weeks thereby fulfilling the definitions of weaning failure [1], or prolonged mechanical ventilation [2]. Such patients are increasingly transferred to specialized respiratory care units when prolonged mechanical ventilation extends beyond the need for acute care [2, 3]. Short-term outcomes from those units have been diverse, likely reflecting the variability in admission and management practices of the different available venues of care [4], but generally reported to be favorable with wean success rates of about 55% within a median time frame of 2 weeks, and around 75% surviving to discharge [4–6]. There is more agreement about the sharply contrasting poor long-term outcomes, with several studies indicating a greater than 50% 1-year mortality [4, 7–12]. There are little available data on the causes of the poor long-term outcomes, which may be related to medical conditions already existing upon admission to these units, to subsequent medical developments, or even to aspects of long-term care. In as much as early correction of potentially modifiable causative factors may favorably impact long-term outcomes, we sought to identify such factors from candidate variables collected during the patients’ stay in a hospital-based respiratory care unit. The association between long-term survival and these variables was analyzed using multiple regression models.
Materials and Methods
Subjects
Between June 2001 and August 2003, 117 mechanically ventilated patients were admitted to the Pulmonary Care Unit (PCU) at Harper University Hospital in Detroit, Michigan, a specialized nine-bed unit for the care of patients with intensive pulmonary needs. Admission criteria included presence of a tracheostomy tube, hemodynamic stability, positive end expiratory pressure ≤8 cmH2O, FiO2 <60%, and failure of wean attempts in the referring ICU. Four patients admitted through that period for a planned brief intervention with known disposition after completion of the intervention were excluded from the cohort. Short-term outcomes on the remaining 113 patients were discussed in a previous report [5]. Of 82 patients discharged alive from the PCU, two patients were discharged to hospice care; the remaining 80 patients are the subjects of the current study. The project was reviewed and approved by the Institutional Review Board of Wayne State University in Detroit, Michigan.
Study Design
The following potential candidate determinants of long-term survival outcomes were collected during the stay in the PCU: age, albumin level on admission to the PCU, severity of illness as determined by the APACHE II score on admission to the PCU, normal or abnormal cardiac ejection fraction (with a cutoff of 50%, if available from a cardiac evaluation within 2 months of admission to the PCU) [13], lung compliance, presence or absence of COPD/emphysema (determined by review of chest radiographs, confirmed history, or documentation by a pulmonologist), presence or absence of any stage sacral decubitus ulcer on admission to the PCU [14], ethnicity (African-American vs. other), gender, length of hospital/ICU stay before admission to the PCU, the rapid shallow breathing index, referral origin of the patient before admission to the PCU (medical vs. surgical), renal function on admission to the PCU (serum creatinine >124 vs. ≤124 μmol/L), and wean status on discharge (weaned vs. not weaned). These were thought to adequately encompass a range of demographic, constitutional, physiologic, pulmonary, and cardiac variables that could be considered of interest in determining long-term survival outcomes. In addition, a subsequent study reported select neuromuscular diseases to be associated with a lower mortality [7]. We accordingly performed a post-hoc analysis reviewing the type of neurologic disease as a potential determinant of long-term survival.
Long-term survival and mortality after discharge were assessed by review of hospital medical records, communications from the primary physicians of record, and review of the United States Social Security Administration Death Master File as of May 15, 2005. This date provided over 2 years of follow-up (757 days) before the first censored data (i.e., all patients of the cohort either died or had at least 757 days of follow-up). Survival was recorded as the number of days from PCU discharge until death or censoring.
Methods
The weaning protocol included therapist-driven protocols, an effort to identify and respond to impediments to weaning in weekly multidisciplinary rounds, formal assessment of readiness to wean, implementation of initial spontaneous breathing trials, and the use of a nonfatiguing form of ventilatory support [2, 5, 15].
Wean success was defined as complete independence from ventilatory support, including noninvasive ventilation, for a full week. Discharge from the PCU was based on successful wean or failure of multiple weans attempts after all potential impediments to wean have been identified and addressed. None of the patients were discharged on noninvasive ventilation modalities.
Lung compliance was measured by dividing the delivered tidal volume in milliliters by the difference between plateau and positive end-expiratory pressures in cmH2O. To obtain a plateau pressure we used the inspiratory hold function of the ventilator for 0.5–1 s and confirmed an adequate plateau by visual inspection of the pressure-time curve on the ventilator display. The rapid shallow breathing index was obtained by dividing the respiratory frequency in breaths per minute by the tidal volume in liters. Tidal volume and respiratory rate were obtained from a hand-held spirometer (Boehringer Laboratories, Norristown, PA) over a minute of spontaneous unassisted breathing with the patient disconnected from the ventilator circuit.
Analysis
Comparison of proportions between groups was done with a χ2 test. Comparison of measures between groups was done with a t test for normally distributed data and the Mann–Whitney test for nonparametric data. Throughout this article we make a specific distinction in our use of the term “survival” in which the number of days until death or censoring is the outcome of interest, and the term “mortality” in which the categorical outcome of death is the outcome of interest.
Survival analyses methods were predominantly used to model our time-to-event data. Specifically, we used Kaplan–Meier estimates to graph the cumulative probability of long-term survival. In addition, for both categorical and continuous variables, Cox proportional regression was used to contrast the relationship between survival and the groups defined by each of the above-described potential predictors of outcome taken individually. Finally, a multivariable Cox proportional regression model was also selected to analyze the association between survival and all significant contributors to long-term survival identified in the preceding analysis.
We used a logistic regression model to evaluate potential determinants of absolute mortality and the Nagelkerke R 2 statistic to assess the strength of the association of the predictor variables with the mortality outcome [16].
The significance level was set at p = 0.05 for all hypotheses. Analyses were performed using SPSS version 11.5.2 (SPSS Inc., Chicago, IL).
Results
General
The median age of the patients was 65 years (mean = 60 years, SD = 17, range = 15–85) (Table 1). Thirteen percent had been discharged home, 24% to a rehabilitation unit, 10% to a nursing home, and 53% to a long-term acute care facility. Other demographic data of interest are reported in Table 1. Fifty-five percent (55%) of patients died within the first year after discharge from the PCU, with a subsequent plateau such that 40% remained alive by the second and third years (Fig. 1). Median hospital/ICU length of stay before admission to the PCU was 19 days in both long-term survivors and nonsurvivors (Mann–Whitney p = 0.55).

Kaplan–Meier curves of survival since discharge from the PCU. Tick marks represent censored patients
Identified impediments to weaning during the stay in the PCU included nutritional deficiency (defined as an albumin level <3.2 g/dl or transferrin level <250 mg/dl) in 81%, presumed active infection in 59%, lung disease (subsuming chronic obstructive pulmonary disease, asthma, obesity hypoventilation, acute respiratory distress syndrome, and interstitial lung disease) in 39%, neurologic disease (subsuming critical care neuropathy or myopathy, motor neurone disease and other neuromuscular diseases, Guillain–Barré syndrome, multiple sclerosis, cerebrovascular accidents, anoxic encephalopathy, and aneurysm surgery) in 29%, and cardiac disease (including coronary artery disease and/or congestive heart failure) in 29%.
Predictors of Long-term Survival and Mortality
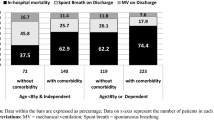
A cutoff age of 65 years was selected for optimal sensitivity and specificity in determining long-term mortality. At that cutoff, 53% of individuals younger than 65 years were alive at the time of assessment (May 2005) compared to only 27.5% of individuals age 65 or above (Pearson χ2 p = 0.02).
The following four categorical variables, listed in order of decreasing hazard ratio (HR), were found to be significant predictors of worse long-term survival: whether the patient was discharged on a ventilator (p = 0.002), presence of a decubitus ulcer on admission to the PCU (p = 0.02), a creatinine level of greater than 124 μmol/L on admission to the PCU (p = 0.02), and age ≥65 years (p = 0.04) (Fig. 2, Table 2). A Cox proportional hazard model incorporating these four variables shows that age ≥65 years, presence of a decubitus ulcer, and discharge while on mechanical ventilation remain independent predictors of worse long-term survival (Table 3). These three variables were similarly found to be significant independent predictors of mortality in a logistic regression model, with a Nagelkerke R 2 of 0.33.

Kaplan–Meier curves of survival since discharge from the PCU stratified by (a) wean status on discharge, (b) skin integrity on admission to the unit, (c) renal function on admission to the unit, (d) age. Tick marks represent censored patients
A post-hoc visual inspection of Kaplan–Meier curves of survival stratified by neurologic diagnosis suggested worse survival in patients with chronic or irreversible neurologic diseases (such as amyotrophic lateral sclerosis or other chronic neuromuscular diseases, multiple sclerosis, stroke, anoxic encephalopathy; together accounting for 28% of patients) compared to those with no neurologic disease or with an acute or reversible disease (such as brain aneurysm surgery, Guillain–Barré syndrome, steroid myopathy, or critical care neuropathy). Specifically, the median survival in patients with chronic or irreversible neurologic disease was 93 days compared to 890 days in those without (HR = 2.4, 95% CI = 1.4–4.4, log rank p = 0.003). Inclusion of this variable in the logistic regression model still showed that type of neurologic disease (odds ratio [OR] = 13.7, 95% CI = 2.3–80, p = 0.004), age (OR = 11.3, 95% CI = 2.6–50, p = 0.001), skin integrity (OR = 8.2, 95% CI = 1.8–37.5, p = 0.007), and wean success (OR = 4.2, 95% CI = 0.95–17.8, p = 0.058) each remained independent variables of interest as predictors of absolute long-term mortality, with a Nagelkerke R 2 of 0.48.
Discussion
The main findings of our study can be summarized as follows:
-
1.
Fifty-five percent (55%) of patients requiring prolonged mechanical ventilation die within the first year after discharge from our PCU, with a subsequent leveling of mortality to 60% by the second and third years. These findings are consistent with other reports [4, 7–11, 17].
-
2.
The following have been individually identified as potential predictors of worse long-term survival: age ≥65 years, the presence of a sacral decubitus ulcer on admission to the unit, a serum creatinine >124 μmol/L on admission to the PCU, and failure to wean off the ventilator prior to discharge.
-
3.
In multivariable models, age, skin integrity, and failure to wean remain independent determinants of long-term survival and mortality.
-
4.
In a post-hoc analysis and in a multivariable model, chronic or irreversible neurologic disease is independently associated with worse long-term survival and mortality.
-
5.
Age, skin integrity, and wean outcome, with or without inclusion of type of neurologic disease, together account for a significant proportion of the variation in the long-term mortality outcomes (Nagelkerke R 2 = 48 and 33%, respectively).
While the specific causes of death of patients discharged from our PCU have not been ascertained in our study, the identification of age, skin integrity, and wean status on discharge as determinants of long-term mortality is important from two standpoints: (1) some of these factors may be modifiable, and (2) cost-effectiveness studies have indicated that the early identification of patients with poor 1-year outcomes may have implications as far as directing intensity of care in such patients [18].
The concordance in the mortality rates across different studies with different approaches and across different long-term care settings [4, 7–11] and the good predictive efficacy of variables identified relatively early in the course of the patients’ illness suggest that other potential contributors to long-term mortality, such as the development of new medical conditions and aspects of long-term care, play a proportionally lesser role.
This study suggests that renal dysfunction and type of neurologic disease are variables of additional interest. However, while both renal dysfunction and stroke have been reported as associated with increased long-term mortality after prolonged mechanical ventilation following cardiac surgery [19], renal dysfunction appears to fall out of significance in our multivariable model, although this may be a limitation of the power of our study.
In contrast, a logistic regression model incorporating type of neurologic disease, wean success, skin integrity, and age shows all four of these variables remain independent predictors of interest, and that all four together account for a significant proportion of the variation in long-term mortality (Nagelkerke R 2 = 48%). This result should be interpreted with caution given the exploratory and post-hoc nature of this latter analysis. Nevertheless, our data are concordant with those of others in showing that neuromuscular conditions such as Guillain–Barré syndrome and ICU myopathy carry a better long-term prognosis [7], but further these findings by indicating that survival may vary between chronic irreversible neurologic conditions and more acute, potentially reversible conditions.
With the exclusion of age, the variables we identify as predictors of long-term survival are potentially modifiable, raising the question of whether interventions that promote weaning success, maintain skin integrity, and possibly prevent renal insufficiency allow improvements in long-term mortality. Therapist-driven weaning protocols [20] and adoption of select ventilatory modalities [21–24] have been longstanding features of the care in our unit [5]. As potential additional strategies, several recent studies from ICU settings suggest that appropriate corticosteroid supplementation for adrenal insufficiency [25], intensive insulin therapy [26], computer-driven protocolized weaning [27], and daily discontinuation of sedation [28] may further enhance liberation from mechanical ventilation. Similarly, intensive insulin therapy has been shown to reduce renal injury [26]. Although none of these measures reduces hospital mortality, our study invites the question as to whether extending these interventions outside the ICU could enhance long-term survival.
Our finding of skin integrity as an independent predictor of long-term survival is concordant with other reports [8, 14], suggesting that closer attention to skin-protective measures is warranted, although whether this translates into reduced long-term mortality remains to be determined. Interestingly, the median hospital length of stay in days before admission to the unit was shorter in patients who had a sacral decubitus ulcer on PCU admission compared to those who did not (14 vs. 20 days respectively, Mann–Whitney test p = 0.04), suggesting that factors other than length of stay predispose the patient to the development of ulcers. While it is likely that a pressure ulcer acts as a surrogate marker of debilitation rather than the proximal cause of death, the specific explanatory power of skin lesions is suggested by our analysis showing it to be independent of age, independent of the presence of immobilizing neurologic conditions, and a better marker than the APACHE II (an index of disease severity) or albumin level (as an index of nutritional balance) in predicting long-term survival. The 36% prevalence of decubitus ulcers in our study is high for hospitalized patients but is at the low-end of the 33–56% range reported for patients such as ours who are coming from intensive care unit settings [29].
Our study differs from other studies in that we could not demonstrate an association between long-term survival and indices of disease severity such as the APACHE II [7–9, 30], ICU length of stay before admission [7], or a diagnosis of COPD [7, 9]. Disease severity scores have been derived and designed in ICU settings, and their accuracy for long-term mortality in a post-intensive-care setting is unclear. Moreover, it is possible that the significance of these indices for prediction of mortality in other studies is due to some subcomponents of their scales, such as age or renal function, already captured in our study. Unlike the study of Pilcher et al. [7], we did not find time spent in the referring ICU to be a predictor of long-term survival, perhaps because the hospital length of stay before admission to our unit was shorter (median of 19 days in our study vs. 26 days in the study of Pilcher et al. [7]). Our inability to find a link between the presence of COPD/emphysema and survival is likely due to variations in patient mix (such as inclusion of any diagnosis of COPD/emphysema in our study rather than COPD as cause of the respiratory failure), heterogeneity of the disease, and the fact that mortality in COPD/emphysema is variable, difficult to predict, and better reflected by surrogate markers of disease severity [31].
Limitations of our study include the relatively small number of patients analyzed, the single-center design, and the unknown cause of death. While some of these limitations may introduce a selection bias, the demographics, severity of illness, surgical vs. medical referral origins, mortality outcomes, and length of stay data of our patients are remarkably comparable to those of other studies in both Europe and the United States [4, 7, 9, 10], thereby providing a good basis for the generalizability of our conclusions. We chose to collect most of the data during the patient’s stay at the respiratory care unit rather than on discharge in order to identify early and modifiable determinants of outcome, and to be concordant with other studies that collected conditions on admission as predictors of outcome [7, 9]. The one exception was the wean outcome measure, which by its nature had to be obtained at discharge. Although this outcome cannot be predicted on admission to a wean unit, it does not preclude interventions to promote wean success as potential means to improve long-term survival.
In conclusion, our study confirms the disappointing long-term survival of patients requiring prolonged mechanical ventilation who survive to discharge from a respiratory care unit. We extend these findings by identifying older age (≥65 years), the presence of a sacral decubitus ulcer on admission to the unit, and persistent respiratory failure as important independent contributing factors to the poor survival. These characteristics together account for a significant proportion of the variance in long-term mortality. Renal dysfunction and chronic irreversible neurologic disease may be additional factors of interest but require further evaluation. Although measures that facilitate weaning, prevent the development of sacral ulcers, and prevent renal dysfunction have not been shown to have impact on short-term mortality, further attention to such interventions is warranted as possible means to improve long-term survival.
References
Simonds AK (2005) Streamlining weaning: protocols and weaning units. Thorax 60:175–182. doi:10.1136/thx.2004.028688
MacIntyre NR, Epstein SK, Carson S, Scheinhorn D, Christopher K, Muldoon S (2005) Management of patients requiring prolonged mechanical ventilation: report of a NAMDRC consensus conference. Chest 128:3937–3954. doi:10.1378/chest.128.6.3937
Corrado A, Roussos C, Ambrosino N, Confalonieri M, Cuvelier A, Elliott M, Ferrer M, Gorini M, Gurkan O, Muir JF, Quareni L, Robert D, Rodenstein D, Rossi A, Schoenhofer B, Simonds AK, Strom K, Torres A, Zakynthinos S, European Respiratory Society Task Force on epidemiology of respiratory intermediate care in Europe (2002) Respiratory intermediate care units: a European survey. Eur Respir J 20:1343–1350. doi:10.1183/09031936.02.00058202
Scheinhorn DJ, Hassenpflug MS, Votto JJ, Chao DC, Epstein SK, Doig GS, Knight EB, Petrak RA, Ventilation Outcomes Study Group (2007) Post-ICU mechanical ventilation at 23 long-term care hospitals: a multicenter outcomes study. Chest 131:85–93. doi:10.1378/chest.06-1081
Aboussouan LS, Lattin CD, Anne VV (2005) Determinants of time-to-weaning in a specialized respiratory care unit. Chest 128:3117–3126. doi:10.1378/chest.128.5.3117
Dasgupta A, Rice R, Mascha E, Litaker D, Stoller JK (1999) Four-year experience with a unit for long-term ventilation (respiratory special care unit) at the Cleveland Clinic Foundation. Chest 116:447–455. doi:10.1378/chest.116.2.447
Pilcher DV, Bailey MJ, Treacher DF, Hamid S, Williams AJ, Davidson AC (2005) Outcomes, cost and long term survival of patients referred to a regional weaning centre. Thorax 60:187–192. doi:10.1136/thx.2004.026500
Seneff MG, Wagner D, Thompson D, Honeycutt C, Silver MR (2000) The impact of long-term acute-care facilities on the outcome and cost of care for patients undergoing prolonged mechanical ventilation. Crit Care Med 28:342–350. doi:10.1097/00003246-200002000-00009
Schonhofer B, Euteneuer S, Nava S, Suchi S, Kohler D (2002) Survival of mechanically ventilated patients admitted to a specialised weaning centre. Intensive Care Med 28:908–916. doi:10.1007/s00134-002-1287-5
Stoller JK, Xu M, Mascha E, Rice R (2003) Long-term outcomes for patients discharged from a long-term hospital-based weaning unit. Chest 124:1892–1899. doi:10.1378/chest.124.5.1892
Elpern EH, Larson R, Douglass P, Rosen RL, Bone RC (1989) Long-term outcomes for elderly survivors of prolonged ventilator assistance. Chest 96:1120–1124. doi:10.1378/chest.96.5.1120
Nava S, Sturani C, Hartl S, Magni G, Ciontu M, Corrado A, Simonds A, European Respiratory Society Task Force on Ethics, decision-making in end stage lung disease (2007) End-of-life decision-making in respiratory intermediate care units: a European survey. Eur Respir J 30:156–164. doi:10.1183/09031936.00128306
Little WC (2001) Assessment of normal and abnormal cardiac function. In: Braunwald E, Zipes DP, Libby P (eds) Heart disease: a textbook of cardiovascular medicine. W.B. Saunders, Philadelphia, pp 479–502
Thomas DR (2001) Prevention and treatment of pressure ulcers: what works? what doesn’t? Cleve Clin J Med 68:704–722
MacIntyre NR, Cook DJ, Ely EW Jr, Epstein SK, Fink JB, Heffner JE, Hess D, Hubmayer RD, Scheinhorn DJ, American College of Chest Physicians, American Association for Respiratory Care, American College of Critical Care Medicine (2001) Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest 120:375S–395S. doi:10.1378/chest.120.6_suppl.375S
Nagelkerke N (1991) A note on a general definition of the coefficient of determination. Biometrika 78:691–692. doi:10.1093/biomet/78.3.691
Cox CE, Carson SS, Lindquist JH, Olsen MK, Govert JA, Chelluri L, Quality of Life After Mechanical Ventilation in the Aged (QOL-MV) Investigators (2007) Differences in one-year health outcomes and resource utilization by definition of prolonged mechanical ventilation: a prospective cohort study. Crit Care 11:R9. 10.1186/cc5667
Cox CE, Carson SS, Govert JA, Chelluri L, Sanders GD (2007) An economic evaluation of prolonged mechanical ventilation. Crit Care Med 35:1918–1927. doi:10.1097/01.CCM.0000275391.35834.10
Engoren M, Buderer NF, Zacharias A (2000) Long-term survival and health status after prolonged mechanical ventilation after cardiac surgery. Crit Care Med 28:2742–2749. doi:10.1097/00003246-200008000-00010
Scheinhorn DJ, Chao DC, Stearn-Hassenpflug M, Wallace WA (2001) Outcomes in post-ICU mechanical ventilation: a therapist-implemented weaning protocol. Chest 119:236–242. doi:10.1378/chest.119.1.236
Brochard L, Rauss A, Benito S, Conti G, Mancebo J, Rekik N, Gasparetto A, Lemaire F (1994) Comparison of three methods of gradual withdrawal from ventilatory support during weaning from mechanical ventilation. Am J Respir Crit Care Med 150:896–903
Ely EW, Baker AM, Dunagan DP, Burke HL, Smith AC, Kelly PT, Johnson MM, Browder RW, Bowton DL, Haponik EF (1996) Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med 335:1864–1869. doi:10.1056/NEJM199612193352502
Esteban A, Frutos F, Tobin MJ, Alia I, Solsona JF, Valverdu I, Fernandez R, de la Cal MA, Benito S, Tomás R (1995) A comparison of four methods of weaning patients from mechanical ventilation. Spanish Lung Failure Collaborative Group. N Engl J Med 332:345–350. doi:10.1056/NEJM199502093320601
Vitacca M, Vianello A, Colombo D, Clini E, Porta R, Bianchi L, Arcaro G, Vitale G, Guffanti E, Lo Coco A, Ambrosino N (2001) Comparison of two methods for weaning patients with chronic obstructive pulmonary disease requiring mechanical ventilation for more than 15 days. Am J Respir Crit Care Med 164:225–230
Huang CJ, Lin HC (2006) Association between adrenal insufficiency and ventilator weaning. Am J Respir Crit Care Med 173:276–280. doi:10.1164/rccm.200504-545OC
Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ, Milants I, Van Wijngaerden E, Bobbaers H, Bouillon R (2006) Intensive insulin therapy in the medical ICU. N Engl J Med 354:449–461. doi:10.1056/NEJMoa052521
Lellouche F, Mancebo J, Jolliet P, Roeseler J, Schortgen F, Dojat M, Cabello B, Bouadma L, Rodriguez P, Maggiore S, Reynaert M, Mersmann S, Brochard L (2006) A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation. Am J Respir Crit Care Med 174:894–900. doi:10.1164/rccm.200511-1780OC
Kress JP, Pohlman AS, O’Connor MF, Hall JB (2000) Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med 342:1471–1477. doi:10.1056/NEJM200005183422002
Peerless JR, Davies A, Klein D, Yu D (1999) Skin complications in the intensive care unit. Clin Chest Med 20:453–467. doi:10.1016/S0272-5231(05)70152-0
Mahul P, Perrot D, Tempelhoff G, Gaussorgues P, Jospe R, Ducreux JC, Dumont A, Motin J, Auboyer C, Robert D (1991) Short- and long-term prognosis, functional outcome following ICU for elderly. Intensive Care Med 17:7–10. doi:10.1007/BF01708401
Cote CG (2006) Surrogates of mortality in chronic obstructive pulmonary disease. Am J Med 119:54–62. doi:10.1016/j.amjmed.2006.08.008
Acknowledgments
The authors gratefully acknowledge Dr. James K. Stoller for his thoughtful review of the manuscript, and the invaluable contributions of the Pulmonary Care Unit nurses, respiratory therapists, and other members of the PCU’s multidisciplinary team. Grant support came from the Department of Internal Medicine, Wayne State University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aboussouan, L.S., Lattin, C.D. & Kline, J.L. Determinants of Long-Term Mortality after Prolonged Mechanical Ventilation. Lung 186, 299–306 (2008). https://doi.org/10.1007/s00408-008-9110-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-008-9110-x