
Abstract
Introduction
Acute supraglottitis is a potentially life-threatening condition that often necessitates intensive care unit (ICU) admission for airway monitoring. The objective of this study was to identify clinical criteria that predict a benign course for patients with acute supraglottitis.
Methods
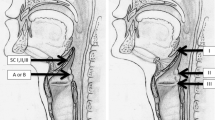
A prospective observational study was performed. Adult patients hospitalized in the ICU between 2007 and 2019 diagnosed with acute supraglottitis were included. All patients were treated with antibiotics and corticosteroids. Fiber optic laryngoscopy (FOL) was performed every 12 h, with each exam defined as “improving”, “no change” or “deteriorating” based on the presence of airway edema. Need for airway intervention was correlated to changes in the FOL exam.
Results
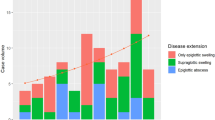
Of 146 patients included, 14 (10%) required intubation, ten on admission, and four during the first 6 h of ICU admission. FOL follow-up was performed on 528 occasions—427 (81%) exams showed improvement, 16 (3%) deterioration, and 85 (16%) with no change. On no occasions was improvement in FOL followed by deterioration. The median ICU length of stay was 3 (IQR 2–3.5) vs. 1 (IQR 1.0–1.25) day for patients who did or did not require intubation (p < 0.001), respectively.
Conclusion
Improvement in FOL exam accurately predicted the absence of need for intubation and might represent a criterion for early ICU discharge.

Similar content being viewed by others

Data availability
Not applicable.
Code availability
Not applicable.
References
Bizaki AJ et al (2011) Acute supraglottitis in adults in Finland: review and analysis of 308 cases. Laryngoscope 121(10):2107–2113
Carenfelt C (1989) Etiology of acute infectious epiglottitis in adults: septic vs. local infection. Scand J Infect Dis 21(1):53–57
Ovnat Tamir S et al (2015) Adult supraglottitis: changing trends. Eur Arch Otorhinolaryngol 272(4):929–935
Ward MA (2002) Emergency department management of acute respiratory infections. Semin Respir Infect 17(1):65–71
Senior BA et al (1994) Changing patterns in pediatric supraglottitis: a multi-institutional review, 1980 to 1992. Laryngoscope 104(11 Pt 1):1314–1322
Shah RK, Roberson DW, Jones DT (2004) Epiglottitis in the Hemophilus influenzae type B vaccine era: changing trends. Laryngoscope 114(3):557–560
Shah RK, Stocks C (2010) Epiglottitis in the United States: national trends, variances, prognosis, and management. Laryngoscope 120(6):1256–1262
Frantz TD, Rasgon BM (1993) Acute epiglottitis: changing epidemiologic patterns. Otolaryngol Head Neck Surg 109(3 Pt 1):457–460
Guldfred LA, Lyhne D, Becker BC (2008) Acute epiglottitis: epidemiology, clinical presentation, management and outcome. J Laryngol Otol 122(8):818–823
Berger G et al (2003) The rising incidence of adult acute epiglottitis and epiglottic abscess. Am J Otolaryngol 24(6):374–383
Carey MJ (1996) Epiglottitis in adults. Am J Emerg Med 14(4):421–424
Park HH et al (2012) Acute supraglottitis in adults: what’s the optimal airway intervention? Auris Nasus Larynx 39(2):204–207
Riffat F et al (2011) Acute supraglottitis in adults. Ann Otol Rhinol Laryngol 120(5):296–299
Phillips JS, Innes AJ, Naik MS (2004) Corticosteroids for supraglottitis. Br J Anaesth 92(3):454–455
Rivron RP, Murray JA (1991) Adult epiglottitis: is there a consensus on diagnosis and treatment? Clin Otolaryngol Allied Sci 16(4):338–344
Shapira Galitz Y et al (2017) Adult acute supraglottitis: analysis of 358 patients for predictors of airway intervention. Laryngoscope 127(9):2106–2112
Friedman M et al (1988) A plea for uniformity in the staging and management of adult epiglottitis. Ear Nose Throat J 67(12):873–874
Hébert PC et al (1998) Adult epiglottitis in a Canadian setting. Laryngoscope 108(1 Pt 1):64–69
Katori H, Tsukuda M (2005) Acute epiglottitis: analysis of factors associated with airway intervention. J Laryngol Otol 119(12):967–972
Park KW, Darvish A, Lowenstein E (1998) Airway management for adult patients with acute epiglottitis: a 12-year experience at an academic medical center (1984–1995). Anesthesiology 88(1):254–261
Mayo-SmithM F et al (1995) Acute epiglottitis. An 18-year experience in Rhode Island. Chest 108(6):1640–1647
Chroboczek T et al (2015) Long-term outcome of critically ill adult patients with acute epiglottitis. PLoS One 10(5):e0125736
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
CS: substantial contributions to conception and design, acquisition of data. Analysis and interpretation of data. Drafting the article, or revising it critically for important intellectual content, final approval of the version to be published. PDL (equal contribution first author). PDA: substantial contributions to conception. Drafting the article content. AR and YS: acquisition of data, analysis, and interpretation of data. J-YS: substantial contributions to concept and design. Substantial contributions to interpretation of data.
Corresponding author
Ethics declarations
Conflict of interest
The authors declared that there was not any financial support. None of the authors has any conflict of interest, financial or otherwise.
Ethical approval
The study was approved by the Institutional Review Board of the Shaare-Zedek Medical Center affiliated with the Hebrew University with a waiver from informed consent requirements.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Chanan Shaul and Philip D. Levin equally contributed to this study.
Rights and permissions
About this article

Cite this article
Shaul, C., Levin, P.D., Attal, P.D. et al. The management of acute supraglottitis patients at the intensive care unit. Eur Arch Otorhinolaryngol 279, 1425–1429 (2022). https://doi.org/10.1007/s00405-021-07174-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-021-07174-w