
Abstract
Purpose
We aimed to evaluate the effectiveness of different antibiotic regimens for the treatment of parapharyngeal abscess (PPA) and characterize patients, who suffered potentially preventable complications (defined as death, abscess recurrence, spread of infection, or altered antibiotic treatment because of insufficient progress).
Methods
Sixty adult patients with surgically verified PPA were prospectively enrolled at five Danish Ear–nose–throat departments.
Results
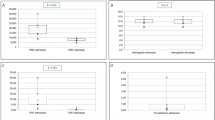
Surgical treatment included internal incision (100%), external incision (13%), and tonsillectomy (88%). Patients were treated with penicillin G ± metronidazole (n = 39), cefuroxime ± metronidazole (n = 16), or other antibiotics (n = 5). Compared to penicillin-treated patients, cefuroxime-treated patients were hospitalized for longer (4.5 vs 3.0 days, p = 0.007), were more frequently admitted to intensive care (56 vs 15%, p = 0.006), underwent external incision more frequently (31 vs 5%, p = 0.018), and suffered more complications (50 vs 18%, p = 0.022), including re-operation because of abscess recurrence (44 vs 3%, p < 0.001). Nine patients suffered potentially preventable complications. These patients displayed significantly higher C-reactive protein levels, received antibiotics prior to admission more frequently, underwent external incision more commonly, and were admitted to intensive care more frequently compared to other patients.
Conclusion
The majority of patients with PPA were effectively managed by abscess incision, tonsillectomy, and penicillin G ± metronidazole. Cefuroxime-treated patients were more severely ill at time of admission and had worse outcome compared to penicillin-treated patients. We recommend penicillin G + metronidazole as standard treatment for patients with PPA, but in cases with more risk factors for potentially preventable complications, we recommend aggressive surgical and broadened antibiotic therapy, e.g. piperacillin–tazobactam.
Similar content being viewed by others


Availability of data and material
Anonymized data can be obtained from the corresponding author upon request.
References
Brito TP, Hazboun IM, Fernandes FL, Bento LR, Zappelini CEM, Chone CT, Crespo AN (2017) Deep neck abscesses: study of 101 cases. Braz J Otorhinolaryngol 83:341–348. https://doi.org/10.1016/j.bjorl.2016.04.004
Oh JH, Kim Y, Kim CH (2007) Parapharyngeal abscess: comprehensive management protocol. ORL J Otorhinolaryngol Relat Spec 69:37–42. https://doi.org/10.1159/000096715
Klug TE, Fischer AS, Antonsen C, Rusan M, Eskildsen H, Ovesen T (2014) Parapharyngeal abscess is frequently associated with concomitant peritonsillar abscess. Eur Arch Otorhinolaryngol 271:1701–1707. https://doi.org/10.1007/s00405-013-2667-x
Alaani A, Griffiths H, Minhas SS, Olliff J, Lee AB (2005) Parapharyngeal abscess: diagnosis, complications and management in adults. Eur Arch Otorhinolaryngol 262:345–350
Daya H, Lo S, Papsin BC, Zachariasova A, Murray H, Pirie J, Laughlin S, Blaser S (2005) Retropharyngeal and parapharyngeal infections in children: the Toronto experience. Int J Pediatr Otorhinolaryngol 69:81–86
Sichel JY, Attal P, Hocwald E, Eliashar R (2006) Redefining parapharyngeal space infections. Ann Otol Rhinol Laryngol 115:117–123
Gianoli GJ, Espinola TE, Guarisco JL, Miller RH (1991) Retropharyngeal space infection: changing trends. Otolaryngol Head Neck Surg 105:92–100
Page C, Chassery G, Boute P, Obongo R, Strunski V (2010) Immediate tonsillectomy: indications for use as first-line surgical management of peritonsillar abscess (quinsy) and parapharyngeal abscess. J Laryngol Otol 124:1085–1090
Woods CR, Cash ED, Smith AM, Smith MJ, Myers JA, Espinosa CM, Chandran SK (2016) Retropharyngeal and parapharyngeal abscesses among children and adolescents in the United States: epidemiology and management trends, 2003–2012. J Pediatric Infect Dis Soc 5:259–268. https://doi.org/10.1093/jpids/piv010
Ohori J, Iuchi H, Nagano H, Umakoshi M, Matsuzaki H, Kurono Y (2020) The usefulness of abscess tonsillectomy followed by intraoral drainage for parapharyngeal abscess concomitant with peritonsillar abscess in the elderly. Auris Nasus Larynx 47:697–701. https://doi.org/10.1016/j.anl.2019.06.003
Sethi DS, Stanley RE (1991) Parapharyngeal abscesses. J Laryngol Otol 105:1025–1030
Thapar A, Tassone P, Bhat N, Pfleiderer A (2008) Parapharyngeal abscess: a life-threatening complication of quinsy. Clin Anat 21:23–26
Klug TE, Greve T, Andersen C, Hahn P, Danstrup C, Petersen NK, Ninn-Pedersen MN, Mikkelsen S, Pauli S, Fuglsang S, Døssing H, Christensen AL, Rusan M, Kjeldsen A (2021) Microbiology of parapharyngeal abscess in adults: in search of the significant pathogens. Eur J Clin Microbiol Infect Dis. https://doi.org/10.1007/s10096-021-04180-y
Versalovic J, Carroll KC, Funke G, Jorgensen JH, Landry ML, Warnock DW. Manual of Clinical Microbiology, 10 Edn. https://doi.org/10.1128/9781555816728
Franzese CB, Isaacson JE (2003) Peritonsillar and parapharyngeal space abscess in the older adult. Am J Otolaryngol 24:169–173
Klug TE (2014) Incidence and microbiology of peritonsillar abscess: the influence of season, age, and gender. Eur J Clin Microbiol Infect Dis 33:1163–1167. https://doi.org/10.1007/s10096-014-2052-8
Sichel JY, Dano I, Hocwald E, Biron A, Eliashar R (2002) Nonsurgical management of parapharyngeal space infections: a prospective study. Laryngoscope 112:906–910
Grisaru-Soen G, Komisar O, Aizenstein O, Soudack M, Schwartz D, Paret G (2010) Retropharyngeal and parapharyngeal abscess in children–epidemiology, clinical features and treatment. Int J Pediatr Otorhinolaryngol 74:1016–1020
Johnston D, Schmidt R, Barth P (2009) Parapharyngeal and retropharyngeal infections in children: argument for a trial of medical therapy and intraoral drainage for medical treatment failures. Int J Pediatr Otorhinolaryngol 73:761–765
Kieff DA, Bhattacharyya N, Siegel NS, Salman SD (1999) Selection of antibiotics after incision and drainage of peritonsillar abscesses. Otolaryngol Head Neck Surg 120:57–61
Wikstén JE, Pitkäranta A, Blomgren K (2016) Metronidazole in conjunction with penicillin neither prevents recurrence nor enhances recovery from peritonsillar abscess when compared with penicillin alone: a prospective, double-blind, randomized, placebo-controlled trial. J Antimicrob Chemother 71:1681–1687. https://doi.org/10.1093/jac/dkw038
Hallgren F, Lindell E, Nilsson-Helger B, Lundqvist A (2021) Antibiotics in treatment of peritonsillar infection: clindamycin versus penicillin. J Laryngol Otol 22:1–6. https://doi.org/10.1017/S002221512100013X
Klug TE, Henriksen JJ, Fuursted K, Ovesen T (2011) Significant pathogens in peritonsillar abscesses. Eur J Clin Microbiol Infect Dis 30:619–627
Øhrstrøm MT, Danstrup CS, Klug TE (2019) Adherence to antibiotic guidelines in the treatment of acute pharyngeal infections. Dan Med J 66:A5530
Acknowledgments
None.
Funding
This work was supported by the Lundbeck Foundation (Grant number: R185-2014–2482), Fonden for lægevidenskabens fremme, and Ørelæge Hans Skovby´s og Hustru Emma Skouby´s Fond.
Author information
Authors and Affiliations
Contributions
TEK: Initiation and design of the study, inclusion of patients, analysis and interpretation of the results, drafting and approval of the manuscript, accountable for all aspects of the work. TG and CA: Design and conduction of microbiological analyses, analysis and interpretation of the results, critical revision, approval of the manuscript, accountable for all aspects of the work. PH, ALC, and AK: Design of the study, inclusion of patients, critical revision, approval of the manuscript; accountable for all aspects of the work. CD, NKP, SM, and HD: Inclusion of patients, critical revision, approval of the manuscript, accountable for all aspects of the work. MR: Analysis and interpretation of the results, critical revision, approval of the manuscript, accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
The authors declared that they have no conflicts of interest.
Ethical approval
The study was approved by the Ethical Committee of Aarhus County (# 1–10-72–4-16).
Consent to participate
Informed consent was obtained from all patients.
Consent for publication
Informed consent was obtained from all patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Klug, T.E., Andersen, C., Hahn, P. et al. Clinical evaluation of antibiotic regimens in patients with surgically verified parapharyngeal abscess: a prospective observational study. Eur Arch Otorhinolaryngol 279, 2057–2067 (2022). https://doi.org/10.1007/s00405-021-06962-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-021-06962-8