
Abstract
Purpose
Adenotonsillectomy is the first-line treatment for pediatric obstructive sleep apnea (OSA). However, although completely resolved OSA after adenotonsillectomy, some children still showed persistence of mouth breathing. Therefore, we attempted to identify risk factors for residual mouth breathing in children with OSA after successful adenotonsillectomy.
Materials and methods
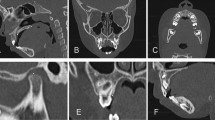
This study retrospectively enrolled children who underwent adenotonsillectomy as a treatment of OSA. Additionally, children who showed apnea–hypopnea index ≥ 1 on 1-year postoperative polysomnography or adenoid regrowth on one-year postoperative lateral cephalogram were excluded. The presence of allergic rhinitis, septal deviation, dentofacial abnormalities, the size of tonsil and adenoid was also evaluated in all enrolled children. Dentofacial abnormalities were defied as a high palatal arch, macroglossia, retrognathia, micrognathia, and overcrowding of teeth which assessed by dentists.
Results
A total of 62 children were enrolled (no residual mouth-breathing group, n = 18 and residual mouth-breathing group, n = 44) in this study. There were no significant differences in demographic factors, physical examination, and sleep parameters, except age and preoperative adenoid size. On the multiple logistic regression analysis, we found that older age, large adenoid size, and presence of dentofacial abnormalities significantly correlated with residual mouth breathing (adjusted coefficient estimates = 0.3890, 2.3611, and 2.8615, respectively) after successful adenotonsillectomy.
Conclusions
Older age, large adenoid size, and presence of dentofacial abnormalities in children with OSA may be the risk factors for residual mouth breathing after successfully resolved OSA.


Similar content being viewed by others
References
Redline S, Tishler PV, Schluchter M, Aylor J, Clark K, Graham G (1999) Risk factors for sleep-disordered breathing in children. Associations with obesity, race, and respiratory problems. Am J Respir Crit Care Med 159(5 Pt 1):1527–1532
Chang SJ, Chae KY (2010) Obstructive sleep apnea syndrome in children: epidemiology, pathophysiology, diagnosis and sequelae. Korean J Pediatr 53(10):863–871
Blunden S, Lushington K, Kennedy D, Martin J, Dawson D (2000) Behavior and neurocognitive performance in children aged 5–10 years who snore compared to controls. J Clin Exp Neuropsychol 22(5):554–568
Urschitz MS, Guenther A, Eggebrecht E et al (2003) Snoring, intermittent hypoxia and academic performance in primary school children. Am J Respir Crit Care Med 168(4):464–468
Li AM, Au CT, Sung RY et al (2008) Ambulatory blood pressure in children with obstructive sleep apnoea: a community based study. Thorax 63(9):803–809
Ramos SD, Mukerji S, Pine HS (2013) Tonsillectomy and adenoidectomy. Pediatr Clin N Am 60(4):793–807
Mitchell RB, Archer SM, Ishman SL et al (2019) Clinical practice guideline: tonsillectomy in children (update). Otolaryngol Head Neck Surg 160(1_suppl):S1–S42
Bhattacharjee R, Kheirandish-Gozal L, Spruyt K et al (2010) Adenotonsillectomy outcomes in treatment of obstructive sleep apnea in children: a multicenter retrospective study. Am J Respir Crit Care Med 182(5):676–683
Friedman M, Wilson M, Lin HC, Chang HW (2009) Updated systematic review of tonsillectomy and adenoidectomy for treatment of pediatric obstructive sleep apnea/hypopnea syndrome. Otolaryngol Head Neck Surg 140(6):800–808
Guilleminault C, Huang YS, Glamann C, Li K, Chan A (2007) Adenotonsillectomy and obstructive sleep apnea in children: a prospective survey. Otolaryngol Head Neck Surg 136(2):169–175
Suri JC, Sen MK, Venkatachalam VP et al (2015) Outcome of adenotonsillectomy for children with sleep apnea. Sleep Med 16(10):1181–1186
Marcus CL, Brooks LJ, Draper KA et al (2012) Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 130(3):e714–e755
Kim JH, Yun S, Hwang SS et al (2018) The 2017 Korean National Growth Charts for children and adolescents: development, improvement, and prospects. Korean J Pediatr 61(5):135–149
Berry RB, Budhiraja R, Gottlieb DJ et al (2010) Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J Clin Sleep Med 8(5):597–619
Friedman M, Ibrahim H, Bass L (2002) Clinical staging for sleep-disordered breathing. Otolaryngol Head Neck Surg 127(1):13–21
Kim SY, Lee WH, Rhee CS, Lee CH, Kim JW (2013) Regrowth of the adenoids after coblation adenoidectomy: cephalometric analysis. Laryngoscope 123(10):2567–2572
Kim DK, Rhee CS, Yun PY, Kim JW (2015) Adenotonsillar hypertrophy as a risk factor of dentofacial abnormality in Korean children. Eur Arch Otorhinolaryngol 272(11):3311–3316
Tauman R, Gulliver TE, Krishna J et al (2006) Persistence of obstructive sleep apnea syndrome in children after adenotonsillectomy. J Pediatr 149(6):803–808
Isaiah A, Hamdan H, Johnson RF, Naqvi K, Mitchell RB (2017) Very severe obstructive sleep apnea in children: outcomes of adenotonsillectomy and risk factors for persistence. Otolaryngol Head Neck Surg 157(1):128–134
Lee SY, Guilleminault C, Chiu HY, Sullivan SS (2015) Mouth breathing, “nasal disuse,” and pediatric sleep-disordered breathing. Sleep Breath 19(4):1257–1264
Huang YS, Guilleminault C (2012) Pediatric obstructive sleep apnea and the critical role of oral-facial growth: evidences. Front Neurol 3:184
Bresolin D, Shapiro PA, Shapiro GG, Chapko MK, Dassel S (1983) Mouth breathing in allergic children: its relationship to dentofacial development. Am J Orthod 83(4):334–340
Zucconi M, Caprioglio A, Calori G et al (1999) Craniofacial modifications in children with habitual snoring and obstructive sleep apnoea: a case-control study. Eur Respir J 13(2):411–417
Kawashima S, Peltomaki T, Sakata H, Mori K, Happonen RP, Ronning O (2002) Craniofacial morphology in preschool children with sleep-related breathing disorder and hypertrophy of tonsils. Acta Paediatr 91(1):71–77
do Nascimento RR, Masterson D, TrindadeMattos C, de Vasconcellos Vilella O (2018) Facial growth direction after surgical intervention to relieve mouth breathing: a systematic review and meta-analysis. J Orofac Orthop 79(6):412–426
Mattar SE, Valera FC, Faria G, Matsumoto MA, Anselmo-Lima WT (2011) Changes in facial morphology after adenotonsillectomy in mouth-breathing children. Int J Paediatr Dent 21(5):389–396
Villa MP, Brasili L, Ferretti A et al (2015) Oropharyngeal exercises to reduce symptoms of OSA after AT. Sleep Breath 19(1):281–289
Rains JC (1995) Treatment of obstructive sleep apnea in pediatric patients. Behavioral intervention for compliance with nasal continuous positive airway pressure. C Clin Pediatr 34(10):535–541
Camacho M, Certal V, Abdullatif J et al (2015) Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep 38(5):669–675
Saccomanno S, Antonini G, D’Alatri L, D’Angelantonio M, Fiorita A, Deli R (2012) Causal relationship between malocclusion and oral muscles dysfunction: a model of approach. Eur J Paediatr Dent 13(4):321–323
Villa MP, Evangelisti M, Martella S, Barreto M, Del Pozzo M (2017) Can myofunctional therapy increase tongue tone and reduce symptoms in children with sleep-disordered breathing? Sleep Breath 21(4):1025–1032
Page DC (2003) “Real” early orthodontic treatment. From birth to age 8. Funct Orthod. 20(1–2):48–54, 56–48
Acknowledgements
We would like to thank Editage (https://www.editage.co.kr) for English language editing.
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any animal studies conducted by the authors. The study was conducted in accordance with the guidelines of the Helsinki Declaration and its subsequent amendments.
Informed consent
Informed consent was not needed; it is a retrospective study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bae, J., Kim, DK. Risk factors for residual mouth breathing in children who had completely resolved obstructive sleep apnea after adenotonsillectomy. Eur Arch Otorhinolaryngol 277, 2913–2919 (2020). https://doi.org/10.1007/s00405-020-06122-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-020-06122-4