
Abstract
Purpose
Diagnostic tonsillectomy is rarely an oncologic operation owing to close or positive margins. The standard of care is for further treatment to the primary site, typically with adjuvant radiotherapy.
Methods
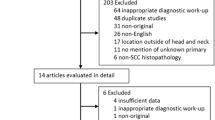
14 patients with close or positive margins following a diagnostic tonsillectomy underwent transoral robotic surgery (TORS) and lateral oropharyngectomy; five patients with the longest follow-up had their excision specimens examined with a step serial sectioning technique (SSS).
Results
Conventional histopathological examination of the TORS resection specimens did not demonstrate residual carcinoma in 13 patients, confirmed by examination using SSS in 5 patients. There were no post-operative complications or long-term functional deficit. Seven patients received surgery alone with 100% overall and disease specific survival, respectively (median follow-up 27.5 months; range 5.2–50.4).
Conclusions
This prospective study suggests that TORS lateral oropharyngectomy alone is an oncologically safe treatment when close or positive margins are identified on diagnostic tonsillectomy in HPV-positive SCC.
Similar content being viewed by others


References
de Almedia JR, Li R, Magnuson JS, Smith R et al (2015) Oncologic outcomes after transoral robotic surgery: a multi-institutional study. JAMA Otolaryngol Head Neck Surg 141(12):1043–1051
Bryan Bell R, Markiewicz M, Dierks EJ, Gregoire CE, Reader A (2013) Thin serial step sectioning of sentinel lymph node biopsy specimen may not be necessary to accurately stage the neck in oral squamous cell carcinoma. J Oral Maxillofac Surg 71:1268–1277
Pytynia KB, Dahlstrom KR, Sturgis EM (2014) Epidemiology of HPV-associated oropharyngeal cancer. Oral Oncol 50(5):380–386
Zapater E, Hernández R, Reboll R, Pérez A, Alba JR, Basterra J (2009) Pathological examination of cordectomy specimens: analysis of negative resection. Auris Nasus Larynx 36:321–325
Helliwel T, Woolgar JA (2013) Dataset for histopathology reporting of muco-sal malignancies of the oral cavity. London: The Royal College of Pathologists. https://www.rcpath.org/resourceLibrary/data-set-for-histopathology-reporting-of-mucosal-malignancies-of-the- oral-cavity.html
Anderson CR, Sisson K, Moncrieff M (2015) A meta-analysis of margin size and local recurrence in oral squamous cell carcinoma. Oral Oncol 51:464–469
Hinni ML, Zarka MA, Hoxworth JM (2013) Margin mapping in transoral surgery for head and neck cancer. Laryngoscope 123:1190–1198
González-Ballester D (2016) The tissue shrinkage phenomenon on surgical margins in oral and oropharyngeal squamous cell carcinoma. Plast Aesthet Res 3:150–157
Hinni ML, Lott DG (2014) Contemporary transoral surgery for primary head and neck cancer. Plural Publishing Inc., San Diego, CA
Sarode G, Sarode SC, Shelke P, Patil S (2017) Histopathological assessment of surgical margins of oral carcinomas and related shrinkage of tumour. Transl Res Oral Oncol 2:1–5
Cheng A, Cox D, Schmidt BL (2008) Oral squamous cell carcinoma margin discrepancy after resection and pathologic processing. J Oral Maxillofac Surg 66:523–529
Sarode SC, Sarode GS (2012) A novel “microscopic method” of shrinkage calculation in the pursuance of shrinkage based histopathologic guidelines for interpretation of surgical margins. Oral Oncol 48:15–16
Mistry RC, Qureshi SS, Kumaran C (2005) Post-resection mucosal margin shrinkage in oral cancer: quantification and significance. J Surg Oncol 91:131–133
Woofer JA, Rogers S, West CR et al (1999) Survival and patterns of recurrence in 200 oral cancer patients treated by radical surgery and neck dissection. Oral Oncol 35:257
Batsakis JG (1999) Surgical excision margins: a pathologist’s perspective. Adv Anat Pathol 6:140
El-Fol HA, Norman SA, Beheiri MG, Khalil AM, Kamel MM (2015) Significance ofresection tissue shrinkage on surgical margins of oral squmous cell carcinoma. J Craniomaxillofacial Surg 43:475–482
Molony P, Kharytaniuk N, Boyle S et al (2017) Impact of positive margins on outcomes of oropharyngeal squamous cell carcinoma according to p16 status. Head Neck 39(8):1680–1688
Amin MB, Edge SB, Greene FL (eds) et al (2017) AJCC cancer staging manual, 8th edn. Springer, New York
Sinha P, Kallogjeri D, Gay H, Thorstad WL, Lewis JS Jr, Chernock R et al (2015) High metastatic node number, not extracapsular spread or N-classification is a node-related prognosticator in transorally-resected, neck-dissected p16-positive oropharynx cancer. Oral Oncol 51:514–520
Roberts TJ, Colevas AD, Hara W, Holsinger FC, Oakley-Girvan I, Divi V (2016) Number of positive nodes is superior to the lymph node ratio and American Joint Committee on Cancer N staging for the prognosis of surgically treated head and neck squamous cell carcinomas. Cancer 122:1388–1397
Ang KK, Harris J, Wheeler R et al (2010) Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med 363(1):24–35
An Y, Holsinger C, Husain ZA (2016) De-intensification of adjuvant therapy in human papillomavirus-associated oropharyngeal cancer. Cancers of Head Neck 1(18):1–9
Sinha P, Lewis JS Jr, Piccirillo JF et al (2012) Extracapsular spread and adjuvant therapy in human papillomavirus-related, p16-positive oropharyngeal carcinoma. Cancer 118:3519–3530
Iyer NG, Dogan S, Palmer F et al (2015) Detailed analysis of clinicopathologic factors demonstrate distinct difference in outcome and prognostic factors between surgically treated HPV-positive and negative oropharyngeal cancer. Ann Surg Oncol 22:4411–4421
Maxwell JH, Ferris RL, Gooding W et al (2013) Extracapsular spread in head and neck carcinoma: impact of site and human papillomavirus status. Cancer 119:3302–3308
Lydiatt WM, Patel SG, O’Sullivan B, Brandwein MS, Ridge JA, Migliacci JC et al (2017) Head and neck cancers—major changes in the American Joint Committee on cancer either edition cancer staging manual. CA Cancer J Clin 67(2):122–137
ClinicalTrials.gov. (2015) Transoral surgery followed by low-dose or standard-dose radiation therapy with or without chemotherapy in treating patients with HPV positive Stage III-IVA oropharyngeal cancer
ClinicalTrials.gov. (2014) Post-operative adjuvant treatment for HPV-positive Tumours (PATHOS)
ClinicalTrials.gov. (2016) Post operative adjuvant therapy de-intensification trial for human papillomavirus-related, p16 + Oropharynx Cancer (ADEPT)
ClinicalTrials.gov. (2016) Radiation therapy and docetaxel in treating patients with HPV-related oropharyngeal cancer
ClinicalTrials.gov: A single-arm phase ii study of post-transoral robotic surgery (TORS) alone to the primary tumor site and selective neck dissection (SND) followed by adjuvant radiation therapy (+/– Chemotherapy) to the Regional nodes for advanced stage, human papilloma virus (HPV) positive, oropharyngeal cancer (2016)
Owen S, Puvanendran M, Meikle D, Bowe I, O’Hara J, Patterson J et al (2016) Baseline swallowing measures predict recovery at 6 weeks after transoral robotic surgery for head and neck cancer. Clin Otolaryngol 42(2):366–372
Stoeckli SJ, Pfaltz M, Ross GL et al (2005) The second international conference on sentinel node biopsy in mucosal head and neck cancer. Ann Surg Oncol 12:919–924
Civantos F, Zitsch R, Bared A, Amin A (2008) Sentinel node biopsy for squamous cell carcinoma of the head and neck. J Surg Oncol 97:683–690
Jefferson GD, Sollaccio D, Gomez-Fernandez CR, Civantos F (2011) Sectioning of sentinel lymph node biopsy in oral squamous cell carcinoma. Otorlayngol Head Neck Surg 144(2):216–219
Sloan P (2009) Head and neck sentinel lymph node biopsy: current state of the art. Head Neck Pathol 3:231–237
Schilling C, Stoeckli SJ, Haerle SK et al (2015) Sentinel European Node Trial (SENT): 3-year results of sentinel node biopsy in oral cancer. Eur J Cancer 51:2777–2784
Hart RD, Nasser JG, Trites JR et al (2005) Sentinel lymph node biopsy in N0 squamous cell carcinoma of the oral cavity and oropharynx. Arch Otolaryngol Head Neck Surg 131:34–38
Halliwell T, Woolgar JA (2011) Standards and datasets for reporting cancers. Dataset for histopathology reporting of mucosal malignancies of the pharynx. Royal College of Pathologists, London
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Siddiq, S., Cartlidge, D., Stephen, S. et al. Robotic lateral oropharyngectomy following diagnostic tonsillectomy is oncologically safe in patients with high risk human papillomavirus related squamous cell cancer. Eur Arch Otorhinolaryngol 275, 1853–1860 (2018). https://doi.org/10.1007/s00405-018-4968-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-018-4968-6