
Abstract
The objective of this article is to evaluate the appropriate timing of tracheostomy in patients with prolonged intubationregarding the incidence of hospital-acquired pneumonia, mortality, length of stay in intensive care unit (ICU) and duration of artificial ventilation. The study included published articles yielded by a search concerning timing of tracheostomy in adult and pediatric patients with prolonged intubation. The search was limited to articles published in English language in the last 30 years (between 1987 and 2017). For the 690 relevant articles, we applied our inclusion and exclusion criteria and only 43 articles were included. 41 studies in the adult age group including 222,501 patients and 2 studies in pediatric age group including 140 patients met our criteria. Studies in adult age group were divided into three groups according to the methodology of determining the cut off timing for early tracheostomy, they were divided into studies that considered early tracheostomy within the first 7, 14 or 21 days of endotracheal intubation, while in pediatric age group the cut off timing for early tracheostomy was within the first 7 days of endotracheal intubation. There was a significant difference in favor of early tracheostomy in adults’ three groups and pediatric age group as early tracheostomy was superior regarding reduced duration of mechanical ventilation, with less mortality rates and less duration of stay in ICU. Regarding hospital-acquired pneumonia, it was significantly less in adult groups but with no significant difference in pediatric age group (3 patients out of 72 pediatric patient with early tracheostomy had pneumonia compared to 11 patients out of 68 with late tracheostomy). Studies defining early tracheostomy as that done within 7 days of intubation had better results than those defining early tracheostomy as that done within 14 or 21 days of intubation. In conclusion, early tracheostomy within 7 days of intubation should be done for both adults and pediatric patients with prolonged intubation.
Similar content being viewed by others
Introduction
Tracheostomy is a frequently performed procedure in about 24% of ICU patients as it has many advantages over prolonged endotracheal intubation as: reducing oropharyngeal and laryngeal trauma, reducing work of breathing by decreasing airway dead space and lowering the airway resistance, improving pulmonary secretion clearance, reducing the use of sedation and decreasing the duration of mechanical ventilation and consequently length of ICU and hospital stay [1, 2]. Open surgical tracheostomy and percutaneous tracheotomy are methods of performing a tracheostomy in selected patients. Open surgical tracheostomy may be required if percutaneous tracheotomy technique is contraindicated due to anatomic or other patient-related problems [2].
The optimal timing of tracheostomy in patients requiring prolonged endotracheal intubation is still a debate despite its advantages. The American National Association of Medical Directors of Respiratory Care in 1989 stated that tracheostomy is indicated if mechanical ventilation is to be continued for more than 21 days while patients requiring mechanical ventilation for less than 10 days are candidates for endotracheal intubation [3]. Other authors recommended early tracheostomy [4] while others mentioned that the evidence of the benefits of tracheostomy over endotracheal intubation is insufficient [5].
The aim of this study is to conduct a meta-analytic study to verify the appropriate timing of tracheostomy in patients with prolonged intubation regarding the incidence of hospital-acquired pneumonia, incidence of mortality, ICU length of stay and duration of mechanical ventilation.
Methods
This study was conducted by searching medical literature in the Medline database with the following keywords: timing of tracheostomy, early versus late tracheostomy and tracheostomy after endotracheal intubation.
The search was limited to articles published in the last 30 years (between 1987 and 2017). in English language to identify prospective, randomized controlled studies assessing the appropriate timing of tracheostomy in prolonged intubated patients. Retrospective studies and studies without control group were excluded. Different tracheostomy techniques either open surgical or percutaneous tracheostomy are included in the study.
Relevant articles were divided into adult and pediatric age groups. Heterogeneity was found due to the difference in defining early and late tracheostomy. So, a sensitivity analysis was conducted dividing the studies in adult age group into three groups according to the methodology of determining the timing of early tracheostomy into studies that considered early tracheostomy within the first 7 days of endotracheal intubation, studies that considered early tracheostomy within 14 days of intubation and studies that considered early tracheostomy within 21 days of intubation.
Each article included was analyzed regarding the methodology and results (type of study, age of patient, number of cases reported in the article, incidence of hospital-acquired pneumonia, incidence of mortality, duration of mechanical ventilation and length of ICU stay). The data collected from each article were statistically analyzed utilizing MedCalc© version 15.8 (MedCalc© Software bvba, Ostend, Belgium).
Studies included in meta-analysis were tested for heterogeneity of the estimates using the following tests:
-
1.
Cochran Q chi square test A statistically significant test (p value < 0.1) denoted heterogeneity among the studies.
-
2.
I-squared (I 2 ) index which is calculated as follows:
(Q Cochran Q chi square test result, \(df\)degree of freedom.
-
3.
The I-squared is interpreted as follows:
0–40%: unimportant heterogeneity; 30–60%: moderate heterogeneity; 50–90%: substantial heterogeneity; 75–100%: considerable heterogeneity.
Results
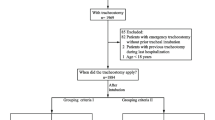
The literature search was performed on 12/2/2017 and yielded 690 articles. Of these 690 articles, there were 647 articles irrelevant to our study from the title and abstract and 43 articles were relevant by meeting our criteria. These 43 studies had 222,641 patients with 41 studies included in adult age group with 222,501 patients and 2 studies included in pediatric age group with 140 patients (Tables 1, 2).
Meta-analysis of studies involving adult patients
Results of comparing early and late tracheostomy in adults regarding hospital-acquired pneumonia:
23 studies were involved including 154,048 patients were divided into three groups according to the timing of early tracheostomy.
I-squared (I 2) index was 83% denoting considerable heterogeneity between studies.
Pooling of estimates via random effects method (REM) showed that all studies regardless of the definition of early and late tracheostomy showed an odds ratio (OR) of 0.68 (95% CI, CL = 0.6–0.77) which was statistically significant (p value < 0.01) favoring early tracheostomy over late tracheostomy regarding incidence of hospital acquired pneumonia.
-
1.
Studies defining early tracheostomy as that done within 7 days Pooling of estimates via REM showed an OR of 0.53 (95% CI, CL = 0.42–0.66) which was statistically significant (p value < 0.01)
-
2.
Studies defining early tracheostomy as that done within 14 days Pooling of estimates via REM showed an OR of 0.78 (95% CI, CL = 0.67–0.9) which was statistically significant (p value < 0.01).
-
3.
Studies defining early tracheostomy as that done within 21 days Only one study showed an OR of 0.29 (95% CI, CL = 0.12–0.75) with statistically significant p value = 0.01.
All favoring early tracheostomy over late tracheostomy regarding incidence of hospital acquired pneumonia.
Comparing the OR of the first two groups showed better OR in studies defining early tracheostomy as that done within 7 days (Fig. 1).

Forest plot for the incidence of hospital-acquired pneumonia (HAP) in adults
Under the random effects model, the point estimate and 95% confidence interval for the combined studies are 0.68 (0.60, 0.77). Using Trim and Fill, these values are unchanged showing no publication bias.
Results of comparing early and late tracheostomy in adults regarding incidence of mortality:
32 studies were involved including 219,727 patients which were divided into three groups according to the timing of early tracheostomy.
I-squared (I 2) index was 83.36% denoting considerable heterogeneity between studies.
Pooling of estimates via random effects method (REM) showed that all studies regardless of the definition of early and late tracheostomy showed an odds ratio (OR) of 0.8 (95% CI, CL = 0.7–0.9) which was statistically significant (p value < 0.01) favoring early tracheostomy over late tracheostomy regarding incidence of mortality in adults.
-
1.
Studies defining early tracheostomy as that done within 7 days Pooling of estimates via REM showed an OR of 0.76 (95% CI, CL = 0.62–0.93) which was statistically significant (p value 0.01).
-
2.
Studies defining early tracheostomy as that done within 14 days Pooling of estimates via REM showed an OR of 0.85 (95% CI, CL = 0.72–0.99) which was statistically significant (p value 0.04).
-
3.
Studies defining early tracheostomy as that done within 21 days Only one study showed an OR of 0.23 (95% CI, CL = 0.09–0.61) with statistically significant p value < 0.01.
All favoring early tracheostomy over late tracheostomy regarding incidence of mortality in adults.
Comparing the OR of the first two groups showed better OR in studies defining early tracheostomy as that done within 7 days (Fig. 2).

Forest plot for mortality in adults
Under the random effects model, the point estimate and 95% confidence interval for the combined studies are 0.80 (0.70, 0.90). Using Trim and Fill, these values are unchanged showing no publication bias.
Results of comparing early and late tracheostomy in adults regarding duration of mechanical ventilation:
22 studies were involved including 4424 patients which were divided into three groups according to the timing of early tracheostomy. I-squared (I 2) index was 98.79% denoting considerable heterogeneity between studies.
Pooling of estimates via random effects method (REM) showed that all studies regardless of the definition of early and late tracheostomy showed a standardized mean difference (SMD) of − 1.06 (95% CI, CL = − 1.3 to − 0.82) which was statistically significant (p value < 0.01) favoring early tracheostomy over late tracheostomy regarding duration of mechanical ventilation in adults.
-
1.
Studies defining early tracheostomy as that done within 7 daysPooling of estimates via REM showed an SMD of − 2.94 (95% CI, CL = − 3.95 to − 1.93) which was statistically significant (p value < 0.01).
-
2.
Studies defining early tracheostomy as that done within 14 daysPooling of estimates via REM showed an SMD of − 0.82 (95% CI, CL = − 1.09 to − 0.55) which was statistically significant (p value < 0.01).
-
3.
Studies defining early tracheostomy as that done within 21 daysOnly one study showed an SMD of − 1.53 (95% CI, CL = − 2.12 to − 0.93) with statistically significant p value < 0.01.
All favoring early tracheostomy over late tracheostomy regarding duration of mechanical ventilation in adults.
Comparing the SMD of the first two groups showed better SMD in studies defining early tracheostomy as that done within 7 days (Fig. 3 ).

Forest plot for the duration of mechanical ventilation (MV) in adults
Under the random effects model, the point estimate and 95% confidence interval for the combined studies are − 1.06 (− 1.3, − 0.82). Using Trim and Fill, these values are unchanged showing no publication bias.
Results of comparing early and late tracheostomy in adults regarding length of stay at the intensive care unit:
27 studies were involved including 143,506 patients which were divided into two groups according to the timing of early tracheostomy.I-squared (I 2) index was 98.99% denoting considerable heterogeneity between studies.
Pooling of estimates via random effects method (REM) showed that all studies regardless of the definition of early and late tracheostomy showed a standardized mean difference (SMD) of − 0.82 (95% CI, CL = − 1.06 to − 0.58) which was statistically significant (p value < 0.01) favoring early tracheostomy over late tracheostomy regarding length of stay at the ICU in adults.
-
1.
Studies defining early tracheostomy as that done within 7 daysPooling of estimates via REM showed an SMD of − 2.61 (95% CI, CL = − 3.44 to − 1.77) which was statistically significant (p value < 0.01).
-
2.
Studies defining early tracheostomy as that done within 14 daysPooling of estimates via REM showed an SMD of − 0.66 (95% CI, CL = − 0.91 to − 0.41) which was statistically significant (p value < 0.01).
Both favoring early tracheostomy over late tracheostomy regarding length of stay at the ICU in adults.
Comparing the SMD of the two groups showed better SMD in studies defining early tracheostomy as that done within 7 days (Fig. 4 ).

Forest plot for the length of stay at the intensive care unit (ICU) in adults
Under the random effects model, the point estimate and 95% confidence interval for the combined studies are − 0.82 (− 1.06, − 0.58). Using Trim and Fill, these values are unchanged showing no publication bias.
Meta-analysis of studies involving pediatric patients
2 studies were involved including 140 patients. 11 patients had early tracheostomy during the first week while 18 patients had late tracheostomy after the first week and 61 patients had early tracheostomy during the second week while 50 patients had late tracheostomy after the second week.
Results of comparing early and late tracheostomy in pediatric patients regarding hospital-acquired pneumonia:
I-squared (I 2) index was 0% denoting no heterogeneity between studies.Pooling of estimates via fixed effects method (FEM) showed that all studies regardless of the definition of early and late tracheostomy showed an odds ratio (OR) of 0.27 (95% CI, CL = 0.06–1.15) which was statistically insignificant (p value = 0.08).Therefore, early tracheostomy is comparable to late tracheostomy regarding incidence of hospital-acquired pneumonia in pediatric age group (Fig. 5 ).

Forest plot for the incidence of hospital-acquired pneumonia (HAP) in pediatric age group
Results of comparing early and late tracheostomy in pediatric patients regarding duration of mechanical ventilation:
I-squared (I 2) index was 0% denoting no heterogeneity between studies.Pooling of estimates via fixed effects method (FEM) showed that all studies regardless of the definition of early and late tracheostomy showed a standardized mean difference (SMD) of − 0.99 (95% CI, CL = − 1.45 to − 0.52) which was statistically significant (p value < 0.01) favoring early tracheostomy over late tracheostomy regarding duration of mechanical ventilation in pediatric age group.
Results of comparing early and late tracheostomy in pediatric patients regarding length of stay at the intensive care unit:
I-squared (I 2) index was 81.27% denoting considerable heterogeneity between studies. Pooling of estimates via random effects method (REM) showed that all studies regardless of the definition of early and late tracheostomy showed a standardized mean difference (SMD) of − 1.65 (95% CI, CL = − 2.85 to − 0.46) which was statistically significant (p value 0.01) favoring early tracheostomy over late tracheostomy regarding length of stay at the ICU in pediatric age group.
Discussion
Although tracheostomy is one of the most frequently performed procedures in ICU patients due to its advantages over prolonged endotracheal intubation, its timing is still a controversy among different authors. There is limited evidence to guide tracheostomy practice.
Many authors found that early tracheostomy reduces the incidence of hospital acquired pneumonia (HAP) in adults because of the reduced airway resistance, which accelerates the weaning process of patients from the ventilator decreasing tracheobronchial colonization and incidence of ventilator-acquired pneumonia [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22]. This agrees with our results where the incidence of HAP was found to be significantly less in patients who had an early tracheostomy done when compared to those with late tracheostomy. Whereas other authors stated that there is no difference between early and late tracheostomy in the incidence of HAP [23,24,25,26,27,28].This may be explained by many factors in different studies. In the study done by Barquist et al. [24], there was a very high incidence of pneumonia in both groups as most of the patients included in the study acquired pneumonia (96.5% in early and 90.3% in late tracheostomy groups) which may have masked the differences between both groups. While the study done by Ahmed and Kuo [23] had insufficient number of patients that decreased the ability to observe a significant difference between the two groups, Zagliet al. [28] considered tracheostomy done after three days to be late tracheostomy; this timing is still considered early by most of the studies in this analysis. While in the study done by Keenan et al. [26], all the participants were trauma patients with different severity and all of them had respiratory failure with unknown comorbidities.
Early tracheostomy reduces the rates of aspiration pneumonia, bacteremia, septic shock, ARDS, and multisystem organ failure. As early tracheostomy decreases length of stay in the ICU, it will decrease the incidence of these ICU-associated complications (which may lead to multisystem organ failure) leading to a reduction in the mortality rate if compared to late tracheostomy in adults [8, 12, 14, 17, 20, 21, 29,30,31,32,33,34,35]. This agrees with our study where themortality rate was significantly less in patients who had early tracheostomy compared to those who had late tracheostomy.
Other authors stated that there is no difference between early and late tracheostomy regarding the mortality rate in adults [6, 10, 11, 14, 18, 19, 23,24,25, 28, 36,37,38,39,40,41,42,43]. Again, the study done by Ahmed and Kuo [23] had insufficient number of patients that lead to the insignificant difference between the two groups and Barquist et al. [24] had small sample size. The low mortality rates reported in the studies done by Arabi et al. [37], Blotet al. [39] and Guanzaet al. [25] considerably reduced the probability of demonstrating the effect of early tracheostomy on prognosis. Only one study done by Keenanet al. [26] suggested that early tracheostomy increases mortality rate. This study had a selection bias regarding different types of injuries and unknown other comorbidities. Study design, severity, and pattern of the disorder, as well as differences in the specialty of the ICUs, caused the debate on the effect of early tracheostomy on mortality.
Early tracheostomy decreases the need for sedation, decreases airway resistance and allows more effective airway secretion suctioning and mouth care; it enhances patient mobility, comfort and ability to speak and eat orally and provides more secure airway control through quicker and safer tube replacement and fixation. This reduces the duration of mechanical ventilation than those with late tracheostomy in adults [6, 7, 9,10,11, 13, 16,17,18, 21, 25, 28, 30, 32, 36, 37, 44, 45]. This goes with our meta-analysis where the duration of mechanical ventilation was found to be significantly less in patients who had an early tracheostomy done when compared to those who had a late tracheostomy.
In spite of this, some authors found no effect of the timing of tracheostomy on the duration of mechanical ventilation [23, 24, 29, 40]. Ahmed and kuo [23] declared less ventilation days with the early group (15.7 ± 6.0 versus 20.0 ± 16.0) but statistically insignificant (p value = 0.570) which may be due to the small number of patients contributed in the study. The study done by Barquistet al. [24] had small sample size and high rate of pneumonia (96.5% in early and 90.3% in late tracheostomy groups) which may influence weaning from mechanical ventilation. The study done by Ben-aviet al. [29] was performed at a tertiary single centre; therefore, these conclusions may not represent global practice. The study done by Boselet al. [40] had heterogeneous small sample size and generalizability was restricted by the single-centre design.
Since early tracheostomy accelerates weaning from mechanical ventilation and reduces aspiration and ventilator-acquired pneumonias, then it enhances the possibility to mobilize patients from the ICU and decreases length of ICU stay than those with late tracheostomy in adults [6,7,8, 10, 11, 13, 16,17,18,19,20,21, 23, 25, 28, 30, 32, 34, 36,37,38, 45, 46]. In our meta-analysis, the length of ICU stay was also found to be significantly less in patients who had an early tracheostomy done when compared to those with late tracheostomy.
While Younget al. [43], Barquistet al. [24], Boselet al. [40] and Ben-aviet al. [29] found that the timing of tracheostomy did not affect the length of ICU stay, Younget al. [43] only included patients at very high risk of prolonged mechanical ventilation due to the absence of a predictive tool to estimate the individual duration of mechanical ventilation, which affected recruitment to the study and the results regarding ICU length of stay. In addition, the study did not recruit its intended sample size due to recruitment fatigue and exhaustion of funding. Again, the small sample size of Boselet al. [40] and Barquistet al. [24] affected their results.
In pediatric age group, Holscheret al. [47] and Leeet al. [48] both suggested a reduction in duration of mechanical ventilation and length of ICU stay in patients with early tracheostomy than those who had late tracheostomy due to the reduction in the amount of sedatives required, increasing patients’ comfort and allowing faster weaning from mechanical ventilator by maintaining more favorable respiratory conditions. However, both studies agreed about no significant difference between both groups regarding incidence of HAP as the incidence of post-tracheostomy pneumonia was similar in both groups. There was a difference in defining early tracheostomy between the two studies as Holscheret al. [47] considered tracheostomy to be early if performed before 7 days of intubation, while Leeet al. [48] considered it early if performed before 14 days of intubation. Less number of studies found concerning tracheostomy in pediatric age might be related to the infrequency of tracheostomy in critically ill children as clinicians prefer more conservative management of the pediatric airway due to the tracheostomy-related complication rate which is approximately 39% [49, 50].
This meta-analysis has some limitations. One of them is the heterogeneity of the data which resulted from the different inclusion and exclusion criteria of each trial, varying patients’ characteristics, tracheostomy techniques, and particularly the different definitions of early and late tracheostomy.We have tried to overcome this heterogeneity through doing a sensitivity analysis according to the methodology of defining early tracheostomy but there were an inevitable overlap between studies defining early tracheostomy within 7, 14, and 21 days of intubation. A second limitation of our analysis is that not all randomized and quasi-randomized trials that compare the outcomes of early tracheostomy with late tracheostomy are included though a thorough search was conducted to minimized missing relevant studies but our search was limited to articles in English language, so, articles in other languages may have been missed. A third limitation is the inability to accurately predict the need for prolonged mechanical ventilation on scientific bases so most of the studies are based on the clinical judgement of the investigators which may carry a selection bias. Another limitation in assessing the pediatric age group was the inability to analyze the mortality rates as there were no sufficient data for conducting a meta-analysis due to paucity of studies. Finally, the patients’ comorbidities and the reason for ICU admission were not available from the studies and could not be analyzed. Future studies on the effect of different tracheostomy techniques on the morbidity in early and late tracheostomies are needed to guide us for the better technique.
Conclusion
Our meta-analysis suggests that in adult patients with prolonged intubation, early tracheostomy is significantly associated with reduction in incidence of hospital acquired pneumonia, incidence of mortality, duration on mechanical ventilation and length of stay in ICU, especially when early tracheostomy is performed within the first 7 days of intubation (according to our sensitivity analysis), while in pediatric age group, early tracheostomy is associated with decreased duration of mechanical ventilation and length of stay in ICU but does not affect the incidence of hospital acquired pneumonia.
References
Frost E (1976) Tracing the tracheostomy. Ann Otolaryngol 85:618–624
Esteban A, Anzueto A, Alia I et al (2000) How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med 161:1450–1458
Plummer A, Gracey D (1989) Consensus conference on artificial airways in patients receiving mechanical ventilation. Chest 96(1):178–1780
Kane T, Rodriguez J, Luchette F (1997) Early versus late tracheostomy in the trauma patient. Respir Care Clin 3:1–20
Maziak D, Meade M, Todd T (1998) The timing of tracheotomy a systematic review. Chest 114:605–609
Alhajhusain A, Ali A, Najmuddin A et al (2014) Timing of tracheotomy in mechanically ventilated critically ill morbidly obese patients. Crit Care Res Pract 2014. https://doi.org/10.1155/2014/840638
Choi HJ, Paeng SH, Kim ST et al (2013) The effectiveness of early tracheostomy (within at least 10 days) in cervical spinal cord injury patients. J Korean Neurosurg Soc 54(3):220–224
Devarajan J, Vydyanathan A, Xu M et al (2012) Early tracheostomy is associated with improved outcomes in patients who require prolonged mechanical ventilation after cardiac surgery. J Am Coll Surg 214:1008–1016
Gessler F, Mutlak H, Lamb S et al (2015) The impact of tracheostomy timing on clinical outcome and adverse events in poor-grade subarachnoid hemorrhage. Crit Care Med 43:2429–2438
Jeon Y, Hwang J, Lim Y et al (2014) Effect of tracheostomy timing on clinical outcome in neurosurgical patients: early versus late tracheostomy. J Neurosurg Anesthesiol 26:22–26
Koch T, Hecker B, Hecker A et al (2012) Early tracheostomy decreases ventilation time but has no impact on mortality of intensive care patients: a randomized study. Langenbeck’s Arch Surg 397(6):1001–1008
Mahafza T, Batarseh S, Bsoul N et al (2012) Early vs. late tracheostomy for the ICU patients: experience in a referral hospital. Saudi J Anaesth 6:152–154
Moller M, Slaikeu J, Bonelli P et al (2005) Early tracheostomy versus late tracheostomy in the surgical intensive care unit. Am J Surg 189(3):293–296
Pinheiro V, Tostes R, Brum C et al (2010) Early vs late tracheostomy in patients with acute severe brain injury. J Bras Pneumol 36:84–91
Rizk E, Patel A, Stetter C et al (2011) Impact of tracheostomy timing on outcome after severe head injury. Neurocrit Care 15:481–489
Rodriguez J, Steinberg S, Luchetti F et al (1990) Early tracheostomy for primary airway management in the surgical critical care setting. Surgery 108(4):655–659
Rumback M, Newton M, Truncale T et al (2004) A prospective, randomized study comparing early percutaneous dilational tracheotomy to prolonged translaryngeal intubation (delayed tracheotomy) in critically ill medical patients. Crit Care Med 32(8):1689–1694
Tong C, Kleinberger A, Paolino J et al (2012) Tracheotomy timing and outcomes in the critically Ill. Otolaryngol–Head Neck Surg 147(1): 44–51
Villwock J, Villwock M, Deshaies E (2014) Tracheostomy timing affects stroke recovery. J Stroke Cerebrovasc Dis 23:1069–1072
Villwock J, Jones K (2014) Outcomes of early versus late tracheostomy: 2008–2010. Laryngoscope 124:1801–1806
Wang H, Lu K, Liliang P et al (2012) The impact of tracheostomy timing in patients with severe head injury: an observational cohort study. Injury 43:1432–1436
Yue Z, Sui F, Chen XK et al (2012) Early versus late percutaneous dilational tracheostomy in critically ill patients anticipated requiring prolonged mechanical ventilation. Chin Med J (Engl) 125:1925–1930
Ahmed N, Kuo Y (2007) Early versus late tracheostomy in patients with severe traumatic head injury. Surg Infect 8(3):343–347
Barquist E, Amortegui J, Hallal A et al (2006) Tracheostomy in ventilator dependent trauma patients: a prospective, randomized intention to treat study. J Trauma 60(1):91–97
Ganuza J, Garcia Forcada A, Gambarrutta C et al (2011) Effect of technique and timing of tracheostomy in patients with acute traumatic spinal cord injury undergoing mechanical ventilation. J Spinal Cord Med 34(1):76–84
Keenan J, Gulack B, Nussbaum D et al (2015) Optimal timing of tracheostomy after trauma without associated head injury. J Surg Res 198(2): 475–481
Terragni P, Antonelli M, Fumagalli R et al (2010) Early vs late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients: a randomized controlled trial. JAMA 303(15):1483–1489
Zagli G, Linden M, Spina R et al (2010) Early tracheostomy in intensive care unit: a retrospective study of 506 cases of video-guided Ciaglia Blue Rhino tracheostomies. J Trauma 68(2):367–372
Ben-Avi R, Ben-Nun A, Levin S et al (2014) Tracheostomy after cardiac surgery: timing of tracheostomy as a risk factor for mortality. J Cardiothorac Vasc Anesth 28:493–496
Bickenbach J, Fries M, Offermanns V et al (2011) Impact of early vs. late tracheostomy on weaning: a retrospective analysis. Minerva Anestesiol 77:1176–1183
Flaatten H, Gjerde S, Heimdal JH et al (2005) The effect of tracheostomy on outcome in intensive care unit patients. Acta Anaesthesiol Scand 50:92–98
Gatti C, Cardu C, Bentini C et al (2004) Weaning from ventilator after cardiac operation using the Ciaglia percutaneous tracheostomy. Eur J Cardiothorac Surg 25:541–547
Hosseinian L, Chianget Y, Itagakial S et al (2013) Earlier versus later tracheostomy in patients with respiratory failure after cardiac surgery in the United States. J Cardiothorac Vasc Anaesth 28(3):488–492
Huang Y, Lee T, Liao C et al (2013) Tracheostomy in craniectomised survivors after traumatic brain injury: a cross-sectional analytical study. Injury 44:1226–1231
Puentes W, Jerath A, Djaiani G et al (2016) Early versus late tracheostomy in cardiovascular intensive care patients. Anaesthesiol Intensive Ther 48(2):89–94
Alali A, Scales D, Fowler R et al (2014) Tracheostomy timing in traumatic brain injury: a propensity-matched cohort study. J Trauma Acute Care Surg 76:70–76
Arabi Y, Haddad S, Shirawi N et al (2004) Early tracheostomy in intensive care trauma patients improves resource utilization: a cohort study and literature review. Critical Care 8(5):347–352
Armstrong P, McCarthy M, Peoples J (1998) Reduced use of resources by early tracheostomy in ventilator-dependent patients with blunt trauma. Surgery 124(4):763–766
Blot F, Similowski T, Trouillet J et al (2008) Early tracheotomy versus prolonged endotracheal intubation in unselected severely ill ICU patients. Intensive Care Med 34(10):1779–1787
Bösel J, Schiller P, Hook Y et al (2012) Stroke-related early tracheostomy versus prolonged orotracheal intubation in neurocritical care trial (SETPOINT): a randomized pilot trial. Stroke 44(1):21–28
Mehta A, Cooke C, Wiener R et al (2016) Hospital variation in early tracheostomy in the United States: a population-based study. Crit Care Med 44(8):1506–1514
Scales D, Thiruchelvam D, Kiss A et al (2008) The effect of tracheostomy timing during critical illness on long-term survival. Critic Care Med 36(9):2547–2557
Young D, Harrison D, Cuthbertson B et al (2013) Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. Caring for the critically Ill patient. JAMA 309(20):2121–2129
Chen H, Song L., Chang H et al (2016) Factors related to tracheostomy timing and ventilator weaning: findings from a population in Northern Taiwan. Clin Respir J 1–8
Hyde G, Savage S, Zarzaur B et al (2014) Early tracheostomy in trauma patients saves time and money. Injury 46(1):110–114
Holloway A, Spaeder M, Basu S (2015) Association of timing of tracheostomy on clinical outcomes in PICU patients. Paediatric Criti Care Med 16(3):52–58
Holscher C, Stewart C, Peltz E et al (2014) Early tracheostomy improves outcomes in severely injured children and adolescents. J Pediatr Surg 49:590–592
Lee J, Koo C, Lee S et al (2016) Effect of early vs. late tracheostomy on clinical outcomes in critically ill pediatric patients. Acta Anaesthesiol Scand 1281–1288
Wood D, McShane P, Davis P (2012) Tracheostomy in children admitted to paediatric intensive care. Arch Dis Child 97: 866–869
Pereira K, Macgregor A, Mcduffie C et al (2003) Tracheostomy in preterm infants: current trends. Arch Otolaryngol Head Neck Surg 129:1268–1271
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
None
Conflict of interest
The authors declare that they have no conflict of interest. The entire work was approved from Ain Shmas University ethical committee.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Adly, A., Youssef, T.A., El-Begermy, M.M. et al. Timing of tracheostomy in patients with prolonged endotracheal intubation: a systematic review. Eur Arch Otorhinolaryngol 275, 679–690 (2018). https://doi.org/10.1007/s00405-017-4838-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-017-4838-7