
Abstract
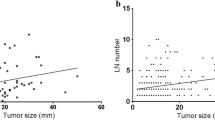
The objective of the present study was to determine the pattern of lymphatic spread in papillary thyroid carcinoma with clinically positive nodes. Between 1999 and 2008, a total of 48 consecutive patients with clinical evidence of cervical lymph node metastasis of papillary thyroid carcinoma underwent 61 modified radical neck dissections (13 being bilateral) including levels II–VI. All neck dissection specimens were separated during surgery into levels and analysis was done with respect to the levels of neck. T value of tumor and demographic parameters were compared with the number of metastatic nodes with univariate analysis. The median number of pathologic nodes in neck dissection specimen was 7.0. The predominant site of metastasis was level VI (77%), followed by level III (69%), level IV (66%), and level II (46%). Level V showed 34% of nodal metastasis. Seven patients had level VII, and five patients had parapharyngeal lymph node dissections because of lymphatic involvement at these sites. There was no statistically significant correlation between T value, age, sex and the number of histologically positive lymph nodes (P = 0.39, P = 0.91 and P = 0.84, respectively). It was concluded that the high incidence of metastatic disease in levels II through VI supports the recommendation for level II through level VI neck dissection in patient with clinically positive neck disease.

Similar content being viewed by others


References
Shaha AR (2004) Implications of prognostic factors and risk groups in the management of differentiated thyroid cancer. Laryngoscope 114:393–402
Caron NR, Clark OH (2005) Papillary thyroid cancer: surgical management of lymph node metastases. Curr Treat Options Oncol 6:311–322
Lundgren CI, Hall P, Dickman PW, Zedenius J (2006) Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case–control study. Cancer 106:524–531
Podnos YD, Smith D, Wagman LD, Ellenhorn JD (2005) The implication of lymph node metastasis on survival in patients with well-differentiated thyroid cancer. Am Surg 71:731–734
Caron NR, Clark OH (2004) Well differentiated thyroid cancer. Scand J Surg 93:261–271
Ito Y, Tomoda C, Uruno T, Takamura Y, Miya A, Kobayashi K et al (2005) Ultrasonographically and anatomopathologically detectable node metastases in the lateral compartment as indicators of worse relapse-free survival in patients with papillary thyroid carcinoma. World J Surg 29:917–920
Kupferman ME, Patterson M, Mandel SJ, LiVolsi V, Weber RS (2004) Patterns of lateral neck metastasis in papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg 130:857–860
Shaha AR (2000) Controversies in the management of thyroid nodule. Laryngoscope 110:183–193
Robbins KT, Clayman G, Levine PA, Medina J, Sessions R, Shaha A et al (2002) Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg 128:751–758
Greene FL, Page DL, Fleming ID et al (2002) AJCC cancer staging manual. Springer, New York
Mazzaferri EL, Jhiang SM (1994) Long term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 97:418–428
Sivanandan R, Soo KC (2001) Pattern of cervical lymph node metastases from papillary carcinoma of the thyroid. Br J Surg 88:1241–1244
Pingpank JF Jr, Sasson AR, Hanlon AL, Friedman CD, Ridge JA (2002) Tumor above the spinal accessory nerve in papillary thyroid cancer that involves lateral neck nodes: a common occurrence. Arch Otolaryngol Head Neck Surg 128:1275–1278
Yanir Y, Doweck I (2008) Regional metastases in well-differentiated thyroid carcinoma: pattern of spread. Laryngoscope 118:433–436
Caron NR, Tan YY, Ogilvie JB, Triponez F, Reiff ES, Kebebew E et al (2006) Selective modified radical neck dissection for papillary thyroid cancer—is level I, II and V dissection always necessary? World J Surg 30:833–840
Koo BS, Yoon YH, Kim JM, Choi EC, Lim YC (2009) Predictive factors of level IIb lymph node metastasis in patients with papillary thyroid carcinoma. Ann Surg Oncol 16:1344–1347
Wada N, Masudo K, Nakayama H, Suganuma N, Matsuzu K, Hirakawa S et al (2008) Clinical outcomes in older or younger patients with papillary thyroid carcinoma: impact of lymphadenopathy and patient age. Eur J Surg Oncol 34:202–207
Machens A, Holzhausen HJ, Lautenschläger C, Thanh PN, Dralle H (2003) Enhancement of lymph node metastasis and distant metastasis of thyroid carcinoma. Cancer 98:712–719
Machens A, Hauptmann S, Dralle H (2009) Lymph node dissection in the lateral neck for completion in central node-positive papillary thyroid cancer. Surgery 145:176–181
Conflict of interest statement
The authors declare that do not have any financial relationship. The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yüce, İ., Çağlı, S., Bayram, A. et al. Regional metastatic pattern of papillary thyroid carcinoma. Eur Arch Otorhinolaryngol 267, 437–441 (2010). https://doi.org/10.1007/s00405-009-1032-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-009-1032-6