
Abstract
Purpose
To examine peri-operative complications in patients undergoing laparoscopic excision of deeply infiltrating endometriosis (DIE).
Methods
This was a prospective study of a case series of women having laparoscopic excision of deeply infiltrating endometriosis from September 2013 through August 2016 in a tertiary referral center for endometriosis and minimally invasive gynaecological surgery in Iran. Data collected included demographics, baseline characteristics, intraoperative and postoperative data up to 1 month following surgery.
Results
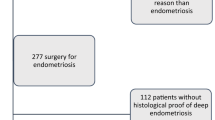
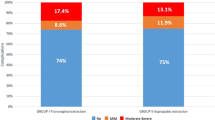
We analysed data from 244 consecutive patients, who underwent radical laparoscopic excision of all visible DIE. Major postoperative complications occurred in 3 (1.2%) and minor complications in 27 (11.1%) of patients. 80.3% of our patient group had Stage IV endometriosis. Segmental bowel resection was performed in 34 (13.9%), disc resection in 7 (2.9%), rectal shave in 53 (21.7%). Joint operating between a gynaecologist and colorectal and/or urological colleague was required in 29.6% of cases. The mean operating time was 223.8 min (± 80.7 standard deviation, range 60–440 min) and mean hospital stay was 2.9 days (± 1.5 standard deviation, range 1–11). The conversion to laparotomy rate was 1.6%.
Conclusions
A combination of different laparoscopic surgical techniques to completely excise all visible DIE, within the context of a tertiary referral center offering multi-disciplinary approach, produces safe outcomes with low complication rates.
Similar content being viewed by others

References
Giudice LC, Kao LC (2004) Endometriosis. Lancet 364:1789–1799
Dunselman GA, Vermeulen N, Becker C, Calhaz-Jorge C, D’Hooghe T, De Bie B, Heikinheimo O, Horne AW, Kiesel L, Nap A, Prentice A, Saridogan E, Soriano D, Nelen W (2014) European society of human reproduction and embryology ESHRE guideline: management of women with endometriosis. Hum Reprod 29:400–412
Minas V, Dada T (2014) Laparoscopic treatment of endometriosis and effects on quality of life: a retrospective study using the short form EHP-5 endometriosis specific questionnaire. J Obstet Gynaecol 34:336–340
Seracchioli R, Mabrouk M, Manuzzi L, Guerrini M, Villa G, Montanari G, Fabbri E, Venturoli S (2008) Importance of retroperitoneal ureteric evaluation in cases of deep infiltrating endometriosis. J Minim Invasive Gynecol 15:435–439
Minelli L, Ceccaroni M, Ruffo G, Bruni F, Pomini P, Pontrelli G, Rolla M, Scioscia M (2010) Laparoscopic conservative surgery for stage IV symptomatic endometriosis: short-term surgical complications. Fertil Steril 94:1218–1222
National Institute for Health and Clinical Excellence (2017) Endometriosis: diagnosis and management. NICE guideline (NG73). https://www.nice.org.uk/guidance/ng73/resources/endometriosis-diagnosis-and-management-pdf-1837632548293
Wolthuis AM, Tomassetti C (2014) Multidisciplinary laparoscopic treatment for bowel endometriosis. Best Pract Res Clin Gastroenterol 28:53–67
Koninckx PR, Ussia A, Adamyan L, Wattiez A, Donnez J (2012) Deep endometriosis: definition, diagnosis, and treatment. Fertil Steril 98:564–571
Donnez J, Jadoul P, Colette S, Luyckx M, Squifflet J, Donnez O (2013) Deep rectovaginal endometriotic nodules: perioperative complications from a series of 3298 patients operated on by the shaving technique. Gynecol Surg 10:31–40
Byrne D, Curnow T, Smith P, Cutner A, Saridogan E, Clark TJ, BSGE Endometriosis Centres (2018) Laparoscopic excision of deep rectovaginal endometriosis in BSGE endometriosis centres: a multicentre prospective cohort study. BMJ Open 8:e018924
Haas D, Wurm P, Shamiyeh A, Shebl O, Chvatal R, Oppelt P (2013) Efficacy of the revised Enzian classification: a retrospective analysis. does the revised Enzian classification solve the problem of duplicate classification in rASRM and Enzian? Arch Gynecol Obstet 287:941–945
Minas V, Gul N, Aust T, Doyle M, Rowlands D (2014) Urinary tract injuries in laparoscopic gynaecological surgery; prevention, recognition and management. Obstet Gynaecol 16:19–28
Kondo W, Bourdel N, Tamburro S, Cavoli D, Jardon K, Rabischong B, Botchorishvili R, Pouly J, Mage G, Canis M (2011) Complications after surgery for deeply infiltrating pelvic endometriosis. BJOG 118:292–298
Donnez J, Squifflet J (2010) Complications, pregnancy and recurrence in a prospective series of 500 patients operated on by the shaving technique for deep rectovaginal endometriotic nodules. Hum Reprod 25:1949–1958
Klugsberger B, Shamiyeh A, Oppelt P, Jabkowski C, Schimetta W, Haas D (2015) Clinical outcome after colonic resection in women with endometriosis. Biomed Res Int 2015:514383
Emmanuel KR, Davis C (2005) Outcomes and treatment options in rectovaginal endometriosis. Curr Opin Obstet Gynecol 17:399–402
Fleisch MC, Xafis D, Bruyne FD, Hucke J, Bender HG, Dall P (2005) Radical resection of invasive endometriosis with bowel or bladder involvement—long-term results. Eur J Obstet Gynecol Reprod Biol 123:224–229
Keckstein J, Wiesinger H (2006) The laparoscopic treatment of intestinal endometriosis. In: Sutton C, Jones K, David Adamson G (eds) Endometriosis. Taylor & Francis, Abingdon, pp 177–187
Meuleman C, D’Hoore A, Van Cleynenbreugel B, Beks N, D’Hooghe T (2009) Outcome after multidisciplinary CO2 laser laparoscopic excision of deep infiltrating colorectal endometriosis. Reprod BioMed Online 18:282–289
Meuleman C, Tomasseti C, D’Hoore A, Buyens A, Van Cleynenbreugel B, Fieuws S, Penninckx F, Vergote I, D’Hooghe T (2011) Clinical outcome after CO2 laser laparoscopic radical excision of endometriosis with colorectal wall invasion combined with laparoscopic segmental bowel resection and reanastomosis. Hum Reprod 26:2336–2343
Abo C, Moatassim S, Marty N, Saint Ghislain M, Huet E, Bridoux V, Tuech JJ, Roman H (2018) Postoperative complications after bowel endometriosis surgery by shaving, disc excision, or segmental resection: a three-arm comparative analysis of 364 consecutive cases. Fertil Steril 109:172–178
Darai E, Ackerman G, Bazot M, Rouzier R, Dubernard G (2007) Laparoscopic segmental colorectal resection for endometriosis: limits and complications. Surg Endosc 21:1572–1577
Meuleman C, Tomassetti C, D’Hoore A, Van Cleynenbreugel B, Penninckx F, Vergote I, D’Hooghe T (2011) Surgical treatment of deeply infiltrating endometriosis with colorectal involvement. Hum Reprod Update 17:311–326
Funding
No external funding was used for this study.
Author information
Authors and Affiliations
Contributions
SK: Project development, Lead surgeon, Manuscript writing and editing, Data analysis. AG: Surgeon, Manuscript writing, Data collection, management and analysis. AM: Database design, project coordination, Data analysis. RK: Surgeon, Data collection. RP: Surgeon, Data collection. KS: Surgeon, Data collection. VM: Data analysis, Manuscript writing and editing
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical approval
All procedures performed were in accordance with the ethical standards of the Ethics Committee of the Avicenna Research Institute, affiliated to the Academic Center for Education, Culture and Research (ACECR) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards (Ethical Committee approval number IR.ACECR.Avicenna.REC.1395.1).
Informed consent
Informed consent was obtained from all patients included in the study. No minors were included in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Khazali, S., Gorgin, A., Mohazzab, A. et al. Laparoscopic excision of deeply infiltrating endometriosis: a prospective observational study assessing perioperative complications in 244 patients. Arch Gynecol Obstet 299, 1619–1626 (2019). https://doi.org/10.1007/s00404-019-05144-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-019-05144-6