
Abstract
Objectives
A previous study demonstrated that the increase in diastolic blood pressure during pregnancy was reduced by supplementation with magnesium. The present study was undertaken to explore if increases in diastolic blood pressure could be useful for early identification of pre-eclampsia.
Study design
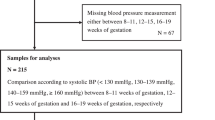
Hospital records of nulliparous, singleton normal pregnancies (n = 100) and those diagnosed with pre-eclampsia (n = 109) were obtained from a register at an antenatal health care unit. Data on blood pressure at the regular visits to the unit were collected and analysed.
Results
The systolic and diastolic blood pressures were significantly higher at pregnancy week 12 among those who developed pre-eclampsia (p = 0.046 and 0.001, resp). An increase in diastolic blood pressure ≥15 mmHg occurred more frequently among women with pre-eclampsia. In 93 % of the cases, this increase was present before and at the same time as the clinical diagnosis of pre-eclampsia was established.
Conclusion
The results suggest that a base-line diastolic blood pressure of ≥80 mmHg and an increase in diastolic blood pressure of ≥15 mmHg could be used to identify women at risk of pre-eclampsia (sensitivity 92 %, specificity 44 %) and as a selection criterion in treatment or prevention assays.




Similar content being viewed by others


References
Gifford RW, August PA, Cunningham G et al (2000) Report of the national high blood pressure program working group on high blood pressure in pregnancy. Am J Obstet Gynecol 183:S1–S22
Backes CH, Markham K, Moorehead P, Cordero L, Nankervis CA, Giannone PJ (2011) Maternal preeclampsia and neonatal outcomes. J Pregnancy. doi:10.1155/2011/214365
Duley L (2009) The global impact of pre-eclampsia and eclampsia. Semin Perinatol 33:130–137
Tranquilli AL, Brown MA, Zeeman GG, Dekker G, Sibai BM (2013) The definition of severe and early-onset preeclampsia. Statements from the international society for the study of hypertension in pregnancy (ISSHP). Pregn Hyperten 3:44–47
Roberts JM, Cooper DW (2001) Pathogenesis and genetics of pre-eclampsia. Lancet 357:53–56
Gilstrap LC III, Ramin SM (2002) Diagnosis and management of preeclampsia and eclampsia. ACOG Pract Bull 33:1–9
Tranquilli AL, Landi B, Giannubilo SR, Sibai BM (2012) Preeclampsia: No longer solely a pregnancy disease. Pregn Hyperten 2:350–357
Fayyad AM, Harrington KF (2005) Prediction and prevention of preeclampsia and IUGR. Early Human Dev 81:865–876
Page EW, Christianson R (1976) The impact of mean arterial pressure in the middle trimester upon the outcome of pregnancy. Am J Obstet Gynecol 125:740–745
Khalil A (2011) First trimester screening for pre-eclampsia. Pregn Hyperten 1:243
Thangaratinam S, Langenveld J, Mol BW, Khan KS (2011) Prediction and primary prevention of pre-eclampsia. Best Pract Res Clin Obstet Gynaecol 25:419–433
Coomarasamy A, Honest H, Papaioannuo et al (2003) Aspirin for prevention of preeclampsia in women with historical risk factors: a systematic review. Obstet Gynecol 101:1319–1332
Hofmeyr GJ, Atllah AN, Duley L (2006) Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev 3:CD0011059
Mello G, Parretti E, Fatini C et al (2005) Low molecular-weight heparin lowers the recurrence rate of preeclampsia and restores the physiological vascular changes in angiotensin-converting enzyme DD women. Hypertension 45:86–91
Duley L, Henderson-Smart D, Meher S, King JF (2007) Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database Syst Rev. doi:10.1002/14651858.CD004659.pub2
Bullarbo M, Ödman N, Nestler A, Nielsen Y, Kolisek M, Vormann J, Rylander R (2013) Magnesium supplementation to prevent high blood pressure in pregnancy—a randomised placebo control trial. Arch Obstet Gynecol 288:1269–1274
Nakamoto O, Tasaka R, Motohisa C (2012) Eclampsia with progressing disease correlates to severe diastolic blood pressure. Pregn Hypertens 2:180
Levine RJ, Ewell MG, Hauth JC et al (2000) Should the definition of preeclampsia include a rise in diastolic blood pressure of ≥15 mm Hg to a level of <90 mm Hg in association with proteinuria? Am J Obstet Gynecol 183:787–792
Gifford RW (2000) Report of the National High Blood Pressure Education Program working group on high blood pressure in pregnancy. Am J Obstet Gynecol 183:S1–S22
Li S, Tian H (1997) Oral low dose magnesium gluconate preventing pregnancy induced hypertension. Chin J Obstet Gynaecol 32:613–615
D’Almeida A, Carter JP, Anatol A, Prost C (1992) Effects of a combination of evening primrose oil (gamma linolenic acid) and fish oil (eicosapentaenoic + doca hexaenoic acid) versus magnesium, and versus placebo in preventing pre-eclampsia. Women Health 19:117–131
Sibai BM, Villar MA, Brazy E (1989) Magnesium supplementation during pregnancy: a double-blind randomized controlled clinical trial. Am J Obstet Gynecol 161:115–119
Acknowledgments
The study was funded by Stiftelsen Swedbank, Sjuhärad, Borås, Sweden.
Conflict of interest
None of the authors has a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bullarbo, M., Rylander, R. Diastolic blood pressure increase is a risk indicator for pre-eclampsia. Arch Gynecol Obstet 291, 819–823 (2015). https://doi.org/10.1007/s00404-014-3476-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-014-3476-1