
Abstract
Background
Epidural anaesthesia (EDA) is an effective method to lower labour pain. EDA might have an impact on instrumental delivery rates and on caesarean section rates. The present study compares the mode of delivery in women who were either receiving EDA or not. The indication for EDA was pain relief only in order to switch off a selection bias.
Methods
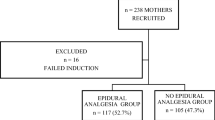
During a 1-year duration, we included a total of 1,452 cases. Exclusion criteria were factors that could influence the mode of delivery, independent from EDA, as well as obstetrical indications for administering EDA. 530 women remained in the analysis. The primary outcome variable was the mode of delivery.
Results
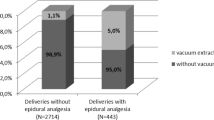
We detected in both nullipara and multipara a statistically significant accumulatin in patients with EDA and caesarean section combined. Most importantly, the majority of the women without EDA (57% of nullipara and 60% of multipara) delivered within the median timeframe from admission until administration of EDA.
Conclusions
It seems to be obvious to conclude that EDA as performed in our study results in a higher rate of caesarean sections. It is important though to take into consideration that between the period from admission to the delivery ward and administration of EDA most of the parturients without EDA had already delivered. Our results make evident, that the administration of EDA exclusively used for reducing labour pain is a result of a complex collaboration of temporal conditions of labour as well as psychological conditions and also of the mother’s wish.


Similar content being viewed by others

References
American College of Obstetricians and Gynecologists Committee on Obstetrics (1993) Committee opinion no 118 pain relief during labor. Int J Gynecol Obstet 42:73
American College of Obstetricians and Gynecologists Committee on Obstetric Practices ACOG (2006) Committee opinion no 339 analgesia and cesarian delivery rates. Obstet Gynecol 107:1487–1488
Anim-Somuah M, Smyth R, Howell C (2006) Epidural versus non-epidural or no analgesia for labour. Cochrane Database Syst Rev 19:CD000331
Aubard Y, Fourgeaud V, Collet D, Grandchamp P, Vincelot A (2003) Forceps delivery and the use of synthetic opioid analgesia during epidural anaesthesia. Eur J Obstet Gynecol Reprod Biol 106:130–133
Chestnut DH, McGrath JM, Vincent RD Jr et al (1994) Does early administration of epidural analgesia affect obstetric outcome in nulliparous women who are in spontaneous labor? Anesthesiology 80:1201–1208
Clark A, Carr D, Loyd G, Cook V, Spinnato J (1998) The influence of epidural analgesia on cesarean delivery rates: a randomized, prospective clinical trial. Am J Obstet Gynecol 179:1527–1533
Eltzschig HK, Lieberman ES, Camann WR (2003) Regional anaesthesia and analgesia for labor and delivery. N Engl J Med 348:319–332
von Eye A (1990) Introduction to configural frequency analysis. University Press, Cambridge
Gomar C, Fernandez C (2000) Epidural analgesia–anaesthesia in obstetrics. Eur Anaesthesiol 17:542–558
Howell CJ (2004) Epidural versus non-epidural analgesia for pain relief in labour (Cochrane review). In: The Cochrane Library, issue 1. Wiley, Chichester
Holm S (1979) A simple sequentially rejective multiple test procedure. Scand J Stat 6:65–70
Hüppe M, Beckhoff M, Klotz KF, Heinzinger M, Prüßmann M, Gerlach K, Ocker H, Schmucker P (2003) Reliabilität und Validität des Anästhesiologischen Nachbefragungsbogens bei elektiv operierten Patienten. Anästhesist 52:311–320
Kinsella SM (2001) Epidural analgesia for labour and instrumental vaginal delivery: an anaesthetic problem with an obstetric solution? Br J Obstet Gynaecol 108:1–2
Krauth J (1993) Einführung in die Konfigurationsfrequenzanalyse (KFA). Weinheim, Beltz
Kuczkowski KM (2004) Ambolatory labor analgesia: What does an obstetrician need to know? Acta Obstet Gynecol Scand 83:415–424
Laux L, Glanzmann P, Schaffner P, Spielberger CD (1981) Das State-Trait-Angstinventar. Weinheim Beltz
Lieberman E, Lang JM, Cohen A, D’Agostino R Jr, Datta S, Frigoletto FD Jr (1996) Association of epidural analgesia with cesarean delivery in nulliparas. Obstet Gynecol 88:993–1000
Nagel B, Gerbershagen HU, Lindena G, Pfingsten M (2002) Entwicklung und empirische Überprüfung des Deutschen Schmerzfragebogens der DGSS. Schmerz 16:263–270
Philipsen T, Jensen NH (1989) Epidural block or parenteral pethidine as analgesic in labour; a randomized study concerning progress in labour and instrumental deliveries. Eur J Obstet Gynecol Reprod Biol 30:27–33
Ramin SM, Gambling DR, Lucas MJ, Sharma SK, Sidawi JE, Leveno KJ (1995) Randomized trial of epidural versus intravenous analgesia during labor. Obstet Gynecol 86:783–789
Rawal N (2005) Combined spinal–epidural anaesthesia. Curr Opin Anaesthesiol 18:518–521
Reynolds F, Dewan D, Morgan B (1992) Ethics and clinical research in obstetric anaesthesia. Lancet 339:1234–1235
Sharma SK, Sidawi JE, Ramin SM, Lucas MJ, Leveno KJ, Cunningham FG (1997) Cesarean delivery: a randomized trial of epidural versus patient-controlled meperidine analgesia during labor. Anesthesiology 87:487–494
Thorp JA, Hu DH, Albin RM et al (1993) The effect of intrapartum epidural analgesia on nulliparous labor: a randomized, controlled, prospective trial. Am J Obstet Gynecol 169:851–858
Von Hundelshausen B (2003) Anästhesie und Analgesie in der Geburtshilfe. Therapeutische Umschau 59:667–676
Zhang J, Yancey MK, Klebanoff MA, Schwarz J, Schweitzer D (2001) Does epidural analgesia prolong labor and increase risk of caesarean delivery? A natural experiment. Am J Obstet Gynecol 185:128–134
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ros, A., Felberbaum, R., Jahnke, I. et al. Epidural anaesthesia for labour: does it influence the mode of delivery?. Arch Gynecol Obstet 275, 269–274 (2007). https://doi.org/10.1007/s00404-006-0248-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-006-0248-6