
Abstract
Introduction
The mechanical conflict in symptomatic femoroacetabular impingement can lead to early osteoarthritis. However, radiographic impingement morphology is often seen in asymptomatic individuals. Long-term observation regarding the risk of developing osteoarthritis in these individuals is lacking. Our study addressed the following questions: Does femoroacetabular impingement morphology increase the risk for development of osteoarthritis after at least 25 years? If yes, which radiographic parameter is the most predictive? Does the level of activity influence the risk for development of osteoarthritis? Are PROM influenced by the grade of osteoarthritis in this population?
Methods
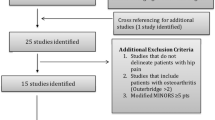
We investigated 51 (32 male, 19 female) patients for whom AP pelvis and Dunn view radiographs were available with a minimum follow-up of 25 years. Alpha angle in AP pelvis and Dunn view radiographs, femoral torsion in Dunn view, lateral center edge angle, cross-over sign, posterior wall sign and prominence of ischial spine sign in AP pelvis radiographs were determined. On the follow-up radiographs, osteoarthritis was graded. Tegner Score for the time of the index radiograph was evaluated. Harris Hip Score and Western Ontario and McMaster Universities Osteoarthritis Index were assessed at latest follow-up.
Results
The mean follow-up was 43 years (range 25–58). Cam impingement morphology showed to increase the risk for development of osteoarthritis: Alpha angles of ≥ 55° on AP pelvis and Dunn view radiographs were associated risk factors and showed an OR of 1.05 (p = 0.002) and 1.10 (p = 0.001), respectively. Abnormal femoral torsion and acetabular retroversion were not risk factors for osteoarthritis. Tegner Score at index presentation, HHS and WOMAC Score did not correlate with the grade of osteoarthritis.
Conclusion
This study showed that cam impingement morphology in young patients raises the risk for development of hip osteoarthritis by 5–10% in a long-term follow-up with a minimum of 25 years, thus its contribution was small.


Similar content being viewed by others


References
Ackerman IN, Bohensky MA, Zomer E et al (2019) The projected burden of primary total knee and hip replacement for osteoarthritis in Australia to the year 2030. BMC Musculoskeletal Disorders 12:84
Agricola R, Waarsing JH, Arden NK et al (2013) Cam impingement of the hip: a risk factor for hip osteoarthritis. Nat Rev Rheumatol 9(10):630–634
Anderson LA, Peters CL, Park BB, Stoddard GJ, Erickson JA, Crim JR (2009) Acetabular cartilage delamination in femoroacetabular impingement Risk factors and magnetic resonance imaging diagnosis. J Bone Joint Surg 34:85
Beck M, Kalhor M, Leunig M, Ganz R (2005) Hip morphology influences the pattern of damage to the acetabular cartilage. J Bone Joint Surg 12:6
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 34:9
Cooperman DR (2019) How Good is the Evidence Linking Acetabular Dysplasia to Osteoarthritis? J Pediatr Orthop 39:S20–S22
de Silva V, Swain M, Broderick C, McKay D (2016) Does high level youth sports participation increase the risk of femoroacetabular impingement? A review of the current literature. Pediatr Rheumatol Online J 14:1–16
Dunn DM (1952) Anteversion of the neck of the femur; a method of measurement. J Bone Joint Surg Br 34(2):181–186
Gala L, Clohisy JC, Beaule PE (2016) Hip dysplasia in the young adult. J Bone Joint Surg Am 98(1):63–73
Ganz R, Leunig M, Leunig-Ganz K, Harris WH (2008) The etiology of osteoarthritis of the hip: an integrated mechanical concept. Clin Orthop Relat R 12:7
Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA (2003) Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat R 34:08
Gosvig KK, Jacobsen S, Sonne-Holm S, Gebuhr P (2008) The prevalence of cam-type deformity of the hip joint: a survey of 4151 subjects of the Copenhagen Osteoarthritis Study. Acta Radiol 49(4):436–441
Grammatopoulos G, Melkus G, Rakhra K, Beaule PE (2019) Does Cartilage Degenerate in Asymptomatic Hips With Cam Morphology? Clin Orthop Relat Res 477(5):962–971
Grantham WJ, Philippon MJ (2019) Etiology and pathomechanics of femoroacetabular impingement. Curr Rev Musculoskelet Med 2:259
Harris WH (1969) Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. J Bone Joint Surg Am 34:09
Hartofilakidis G, Bardakos NV, Babis GC, Georgiades G (2011) An examination of the association between different morphotypes of femoroacetabular impingement in asymptomatic subjects and the development of osteoarthritis of the hip. J Bone Joint Surg Br 93(5):580–586
Issa SN, Sharma L (2006) Epidemiology of osteoarthritis: an update. Curr Rheumatol Rep 24:05
Jung KA, Restrepo C, Hellman M, AbdelSalam H, Morrison W, Parvizi J (2011) The prevalence of cam-type femoroacetabular deformity in asymptomatic adults. J Bone Joint Surg Br 93(10):1303–1307
Kalberer F, Sierra RJ, Madan SS, Ganz R, Leunig M (2008) Ischial spine projection into the pelvis : a new sign for acetabular retroversion. Clin Orthop Relat Res 466(3):677–683
Kapron AL, Aoki SK, Peters CL, Anderson AE (2014) Subject-specific patterns of femur-labrum contact are complex and vary in asymptomatic hips and hips with femoroacetabular impingement. Clin Orthop Relat R 65:02
Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheumatic Diseases 98:28
Lawrence RC, Felson DT, Helmick CG et al (2008) Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Arthritis Rheumat 567:91–174
Lee CB, Spencer HT (2017) Comparison of intraoperative fluoroscopic dunn view with magnetic resonance imaging to determine femoral version. Arthroscopy 33(6):1186–1193
Lequesne M (1963) Coxometry measurement of the basic angles of the adult radiographic hip by a combined protractor. Rev Rhum Mal Osteoartic 30:479–485
Lysholm J, Gillquist J (1982) Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 54:02
Murphy LB, Helmick CG, Schwartz TA et al (2010) One in four people may develop symptomatic hip osteoarthritis in his or her lifetime. Osteoarthritis Cartilage 18(11):1372–1379
Murphy SB, Ganz R, Muller ME (1995) The prognosis in untreated dysplasia of the hip. A study of radiographic factors that predict the outcome. J Bone Joint Surg Am 77:985–989
Nevitt MC, Lane NE, Scott JC et al (1995) Radiographic osteoarthritis of the hip and bone mineral density. The Study of Osteoporotic Fractures Research Group, Arthritis and rheumatism
Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J (2002) The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br 84(4):556–560
Parvizi J, Leunig M, Ganz R (2007) Femoroacetabular impingement. J Am Acad Orthop Surg 15(9):561–570
Reynolds D, Lucas J, Klaue K (1999) Retroversion of the acetabulum. A cause of hip pain. J Bone Joint Surg Br 81:281–288
Rippstein J (1955) Determination of the antetorsion of the femur neck by means of two x-ray pictures. Z Orthop Ihre Grenzgeb 86(3):345–360
Saberi Hosnijeh F, Zuiderwijk ME, Versteeg M et al (2017) Cam deformity and acetabular dysplasia as risk factors for hip osteoarthritis. Arthrit Rheumatol 43:75
Smith-Petersen MN (2009) The classic: treatment of malum coxae senilis, old slipped upper femoral epiphysis, intrapelvic protrusion of the acetabulum, and coxa plana by means of acetabuloplasty 1936. Clin Orthop Relat Res 467:608–615
Speirs AD, Beaulé PE, Huang A, Frei H (2017) Properties of the cartilage layer from the cam-type hip impingement deformity. J Biomech 65:84
Sutter R, Dietrich TJ, Zingg PO, Pfirrmann CW (2012) Femoral antetorsion: comparing asymptomatic volunteers and patients with femoroacetabular impingement. Radiology 263(2):475–483
Sutter R, Dietrich TJ, Zingg PO, Pfirrmann CW (2012) How useful is the alpha angle for discriminating between symptomatic patients with cam-type femoroacetabular impingement and asymptomatic volunteers? Radiology 264(2):514–521
Tannast M, Fritsch S, Zheng G, Siebenrock KA, Steppacher SD (2015) Which radiographic hip parameters do not have to be corrected for pelvic rotation and tilt? Clin Orthop Relat Res 473(4):1255–1266
Tegner Y, Lysholm J (1985) Tegner score. Clin Orthop Relat Res 65:1–86
Thomas GER, Palmer AJR, Batra RN et al (2014) Subclinical deformities of the hip are significant predictors of radiographic osteoarthritis and joint replacement in women. A 20 year longitudinal cohort study. Osteoarth artilage 547:96–123
Tonnis D (1990) Surgical treatment of congenital dislocation of the hip. Clin Orthop Relat Res 258:33–40
Toogood PA, Skalak A, Cooperman DR (2009) Proximal femoral anatomy in the normal human population. Clin Orthop Relat Res 467(4):876–885
Werner CM, Copeland CE, Ruckstuhl T et al (2010) Radiographic markers of acetabular retroversion: correlation of the cross-over sign, ischial spine sign and posterior wall sign. Acta Orthop Belg 76(2):166–173
Wyles CC, Heidenreich MJ, Jeng J, Larson DR, Trousdale RT, Sierra RJ (2017) The John Charnley award: Redefining the Natural History of Osteoarthritis in patients with hip dysplasia and impingement. Clin Orthop Relat 36:79
Wyles CC, Norambuena GA, Howe BM et al (2017) Cam deformities and limited hip range of motion are associated with early osteoarthritic changes in adolescent athletes: a prospective matched cohort study. Am J Sports Med 45(13):3036–3043
Acknowledgments
We thank Christa Fritschi, UCAR, Balgrist University Hospital for her assistance in this research project
Funding
There is no funding source.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The local ethical committee approved this study (Zurich Cantonal Ethics Commission, 2017–00840).
Informed consent
All patients gave their informed consent for their participation in and the publication of this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hoch, A., Schenk, P., Jentzsch, T. et al. FAI morphology increases the risk for osteoarthritis in young people with a minimum follow-up of 25 years. Arch Orthop Trauma Surg 141, 1175–1181 (2021). https://doi.org/10.1007/s00402-020-03522-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-020-03522-3