
Abstract
Introduction
The minimally invasive direct anterior approach (DAA) is an established approach for primary total hip arthroplasty (THA). The complication rates in hip revision arthroplasty are much higher in comparison with primary THA. A right positioning of the implants and a soft tissue, especially the abductors spearing approach, is important to get good functional results and low complication rates. The aim of this study was to show the clinical and radiological outcome of isolated revision hip arthroplasty of the cup by using the DAA.
Materials and methods
Aseptic cup revisions were carried out in 48 patients using the DAA. A decision to exchange the stem was made intraoperatively in seven cases. Complications, radiological and functional outcome were assessed. All of the data were collected retrospectively. The mean follow-up period was 65 months.
Results
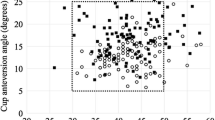
In most of the cases the standard DAA was used. A proximal extension was nescessary in 15 patients (31%). The mean cup inclination angle after revision was 44° (min. 25°, max. 62°). Six implants (12.5%) were located outside of the Lewinnek safe zone. The centers of rotation of the revision implants were a mean of 0.6 cm superior (min. 0, max. 2.2 cm) and 0.5 cm lateral (min. 0.2 cm, max 1.2 cm) in comparison with the center of rotation in the healthy hip on the contralateral side. Harris Hip Score improved significantly from 50 to 91 (P = 0.03). Complications noted consisted of two periprosthetic infections (4.2%), one aseptic cup loosening (2.1%), two hematomas requiring revision (4.2%), and one case each of femoral nerve injury, lower-leg venous thrombosis, and pneumonia. No dislocations were observed and there were no cases of heterotopic ossification based on the Brooker classification. No persistent damage of the nervus cutaneus femoris lateralis was found at the follow-up examinations.
Conclusions
The DAA represents a feasible option in hip revision arthroplasty. Anatomic reconstruction of the cup is reproducibly possible. Good medium-term results can also be achieved. Particularly in relation to dislocation, the complication rates are low. Due to the learning curve, the DAA should only be used in hip revision arthroplasty by those with sufficient experience in primary THA. Adequate data regarding stem revisions through the DAA are not available at the moment.
Similar content being viewed by others


References
Meermans G, Konan S, Das R, Volpin A, Haddad FS (2017) The direct anterior approach in total hip arthroplasty: a systematic review of the literature. Bone Joint J 99–B:732–740
Christensen CP, Jacobs CA (2015) Comparison of patient function during the first six weeks after direct anterior or posterior total hip arthroplasty (THA): a randomized study. J Arthroplasty 30:94–97
Meneghini RM, Pagnano MW, Trousdale RT, Hozack WJ (2006) Muscle damage during MIS total hip arthroplasty: Smith-Petersen versus posterior approach. Clin Orthop 453:293–298
Müller M, Tohtz S, Dewey M, Springer I, Perka C (2010) Evidence of reduced muscle trauma through a minimally invasive anterolateral approach by means of MRI. Clin Orthop 468:3192–3200
Barrett WP, Turner SE, Leopold JP (2013) Prospective randomized study of direct anterior vs postero-lateral approach for total hip arthroplasty. J Arthroplasty 28:1634–1638
Hoell S, Sander M, Gosheger G, Ahrens H, Dieckmann R, Hauschild G (2014) The minimal invasive direct anterior approach in combination with large heads in total hip arthroplasty—is dislocation still a major issue? A case control study. BMC Musculoskelet Disord 15:80
Tsukada S, Wakui M (2015) Lower dislocation rate following total hip arthroplasty via direct anterior approach than via posterior approach: five-year-average follow-up results. Open Orthop J 9:157–162
Newman EA, Holst DC, Bracey DN, Russell GB, Lang JE (2016) Incidence of heterotopic ossification in direct anterior vs posterior approach to total hip arthroplasty: a retrospective radiographic review. Int Orthop 40:1967–1973
Badarudeen S, Shu AC, Ong KL, Baykal D, Lau E, Malkani AL (2017) Complications after revision total hip arthroplasty in the Medicare population. J Arthroplasty 32:1954–1958
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR (1978) Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am 60:217–220
Babis GC, Sakellariou VI, Chatziantoniou AN, Soucacos PN, Megas P (2011) High complication rate in reconstruction of Paprosky type IIIa acetabular defects using an oblong implant with modular side plates and a hook. J Bone Joint Surg Br 93:1592–1596
Meermans G, Haddad FS (2010) Is there a role for tissue biopsy in the diagnosis of periprosthetic infection? Clin Orthop 468:1410–1417
Rachbauer F, Krismer M (2008) Minimally invasive total hip arthroplasty via direct anterior approach. Oper Orthopadie Traumatol 20:239–251
Putzer D, Haselbacher M, Hörmann R, Klima G, Nogler M (2017) The deep layer of the tractus iliotibialis and its relevance when using the direct anterior approach in total hip arthroplasty: a cadaver study. Arch Orthop Trauma Surg 137(12):1755–1760
Mast NH, Laude F (2011) Revision total hip arthroplasty performed through the Hueter interval. J Bone Joint Surg Am 93(Suppl 2):143–148
DeLee JG, Charnley J (1976) Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop 121:20–32
Brooker AF, Bowerman JW, Robinson RA, Riley LH (1973) Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am 55:1629–1632
Lee GC, Marconi D (2015) Complications following direct anterior hip procedures: costs to both patients and surgeons. J Arthroplasty 30:98–101
Mjaaland KE, Svenningsen S, Fenstad AM, Havelin LI, Furnes O, Nordstetten L (2017) Implant survival after minimally invasive anterior or anterolateral vs. conventional posterior or direct lateral approach: an analysis of 21,860 total hip arthroplasties from the Norwegian Arthroplasty Register (2008–2013). J Bone Joint Surg Am 99:840–847
Ponzio DY, Poultsides LA, Salvatore A, Lee YY, Memtsoudis SG, Alexiades MM (2018) In-hospital morbidity and postoperative revisions after direct anterior vs posterior total hip arthroplasty. J Arthroplasty 33(5):1421–1425. https://doi.org/10.1016/j.arth.2017.11.053
De Geest T, Fennema P, Lenaerts G, De Loore G (2015) Adverse effects associated with the direct anterior approach for total hip arthroplasty: a Bayesian meta-analysis. Arch Orthop Trauma Surg 135(8):1183–1192
Soderquist MC, Scully R, Unger AS (2017) Acetabular placement accuracy with the direct anterior approach freehand technique. J Arthroplasty 32:2748–2754
Kawarai Y, Iida S, Nakamura J, Shinada Y, Suzuki C, Ohtori S (2017) Does the surgical approach influence the implant alignment in total hip arthroplasty? Comparative study between the direct anterior and the anterolateral approaches in the supine position. Int Orthop 41:2487–2493
Kiyama T, Naito M, Shitama H, Maeyama A (2009) Effect of superior placement of the hip center on abductor muscle strength in total hip arthroplasty. J Arthroplasty 24:240–245
Pagnano W, Hanssen AD, Lewallen DG, Shaughnessy WJ (1996) The effect of superior placement of the acetabular component on the rate of loosening after total hip arthroplasty. J Bone Joint Surg Am 78:1004–1014
Asayama I, Chamnongkich S, Simpson KJ, Kinsey TL, Mahoney OM (2005) Reconstructed hip joint position and abductor muscle strength after total hip arthroplasty. J Arthroplasty 20:414–420
Spanyer JM, Beaumont CM, Yerasimides JG (2017) The extended direct anterior approach for column augmentation in the deficient pelvis: a novel surgical technique, and case series report. J Arthroplasty 32:515–519
Gehrke T, Bangert Y, Schwantes B, Gebauer M, Kendoff D (2013) Acetabular revision in THA using tantalum augments combined with impaction bone grafting. Hip Int 23:359–365
von Roth P, Abdel MP, Wauer F, Winkler T, Wassilew G, Diederichs G, Perka C (2014) Significant muscle damage after multiple revision total hip replacements through the direct lateral approach. Bone Joint J 96–B:1618–1622
Kawasaki M, Hasegawa Y, Okura T, Ochiai S, Fujibayashi T (2017) Muscle damage after total hip arthroplasty through the direct anterior approach for developmental dysplasia of the hip. J Arthroplasty 32:2466–2473
Cogan A, Klouche S, Mamoudy P, Sariali E (2011) Total hip arthroplasty dislocation rate following isolated cup revision using Hueter’s direct anterior approach on a fracture table. Orthop Traumatol Surg Res 97:501–505
Bouveau V, Haen TX, Poupon J, Nich C (2018) Outcomes after revision of metal on metal hip resurfacing to total arthroplasty using the direct anterior approach. Int Orthop 42(11):2543–2548
Mayr E, Krismer M, Ertl M, Kessler O, Thaler M, Nogler M (2006) Uncompromised quality of the cement mantle in Exeter femoral components implanted through a minimally-invasive direct anterior approach. A prospective, randomised cadaver study. J Bone Joint Surg Br 88(9):1252–1256
Ghijselings SGM, Driesen R, Simon JP, Corten K (2017) Distal extension of the anterior approach to the hip using the femoral interbundle technique: surgical technique and case series. J Arthroplasty 32(7):2186–2190
Ghijselings SG, Driesen R, Simon JP, Corten K (2017) Distal extension of the direct anterior approach to the hip: a cadaveric feasibility study. J Arthroplasty 32(1):300–303
Nogler MM, Thaler MR, The Direct Anterior Approach for Hip Revision (2017) Accessing the entire femoral diaphysis without endangering the nerve supply. J Arthroplasty 32(2):510–514
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Horsthemke, M.D., Koenig, C., Gosheger, G. et al. The minimalinvasive direct anterior approach in aseptic cup revision hip arthroplasty: a mid-term follow-up. Arch Orthop Trauma Surg 139, 121–126 (2019). https://doi.org/10.1007/s00402-018-3062-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-018-3062-2