
Abstract
Background
Rehabilitation is one of the most critical points after anterior cruciate ligament (ACL) reconstruction. However, the recent trend of low-cost, short-term hospitalization makes sufficient rehabilitation after ACL reconstruction difficult.
Patients and methods
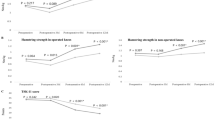
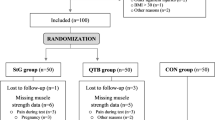
Level of evidence III: 34 patients who underwent non-anatomical single bundle ACL reconstruction using a hamstring auto graft were evaluated. Twenty patients (12 males and 8 females) were transferred to a special rehabilitation hospital (RH hospital group) after operation and concentrated rehabilitation was performed up to 4 h per day. Fourteen (9 males and 5 females) patients performed clinic-based rehabilitation at a university hospital three times per week (clinic group). Strength of quadriceps and knee flexion muscles was assessed at 60°/s using a Cybex II dynamometer (Lumex, Ronkonkoma, NY, USA) at 3, 6 and 9 months after ACL reconstruction. Anterior tibial translation (ATT) and pivot shift test were also evaluated.
Results
No significant difference in muscle recovery in the lower extremity was observed at any time point after ACL reconstruction between the clinic group and the RH hospital group. However, 3 months after operation, the average muscle strength of the RH hospital group tended to be higher than that of the clinic group. There was no significant difference in ATT or pivot shift (each group included 4 positive pivot shift subjects) in the patients who were tested between the clinic group and the RH hospital group.
Conclusion
Concentrated rehabilitation at a rehabilitation hospital after ACL reconstruction has the potential to improve muscle strength in the lower extremities more dramatically in the early stages of post operation. However, the initial benefits of intensive physiotherapy disappear after 6 months.



Similar content being viewed by others

Abbreviations
- ACL:
-
Anterior cruciate ligament
- ATT:
-
Anterior tibial translation
- RH:
-
Rehabilitation
References
Muneta T, Sekiya I, Ogiuchi T, Yagishita K, Yamamoto H, Shinomiya K (1998) Effects of aggressive early rehabilitation on the outcome of anterior cruciate ligament reconstruction with multi-strand semitendinosus tendon. Int Orthop 22:352–356
Beynnon BD, Ur BS, Johnson RJ et al (2005) Rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind comparison of programs administrated over 2 different time intervals. Am J Sports Med 33:347–359
Keays SL, Bullock-Saxton J, Keays AC (2000) Strength and function before and after anterior cruciate ligament reconstruction. Clin Orthop Relat Res 373:174–183
de Jong SN, van Caspel DR, van Haeff MJ, Saris DB (2007) Functional assessment and muscle strength before and after reconstruction of chronic anterior cruciate ligament lesions. Arthroscopy 23:21–28
Eitzen I, Holm I, Risberg MA (2009) Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction. Br J Sports Med 43:371–376
Myer GD, Ford KR, Barber Foss KD, Liu C, Nick TG, Hewett TE (2009) The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med 19:3–8
Wright R, Preston E, Fleming BC et al (2008) A systematic review of anterior cruciate ligament reconstruction rehabilitation. J Knee Surg 21:225–234
Feller JA, Webstar KE, Gavin B (2001) Early post-operative morbidity following anterior cruciate ligament reconstruction: patellar tendon versus hamstring graft. Knee Surg Sports Traumatol Arthrosc 9:260–266
Kobayashi A, Higuchi H, Terauchi M, Kobayashi F, Kimura M, Takagishi K (2004) Muscle performance after anterior cruciate ligament reconstruction. Int Orthop 28:48–51
Witvrouw E, Bellemans R, Verdonk R, Cambier D, Coorevits F, Almqvist F (2001) Patellar tendon vs. doubled semitendinosus and gracilis tendon for anterior cruciate ligament reconstruction. Int Orthop 25:308–311
Isberg J, Faxen E, Brandsson S, Eriksson BI, Karrholm J, Karlsson J (2006) Early active extension after anterior cruciate ligament reconstruction does not result in increased laxity of the knee. Knee Surg Sports Traumatol Arthrosc 14:1108–1115
Shelbourne KD, Klots C (2006) What I have learned about the ACL: utilizing a progressive rehabilitation scheme to achieve total knee symmetry after anterior cruciate ligament reconstruction. J Orthop Sci 11:318–325
Alenton-Geri E, Myer GD, Silvers HJ et al (2009) Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 2: a review of prevention programs aimed to modify risk factors and to reduce injury rates. Knee Surg Sports Traumatol Arthrosc 17:859–879
Lim BO, Lee YS, Kim JG, An KO, Yoo J, Kwon YH (2009) Effects of sports injury prevention training on the biomechanical risk factors of anterior cruciate ligament injury in high school female basketball players. Am J Sports Med 37:1728–1734
Acknowledgments
Professor Akiyoshi Saito, Dr. Shigeru Suzuki and physical therapists who are working at Surugadai Nihon University hospital and Kamimoku hot springs hospital are greatly acknowledged for their kind assistance on this study.
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iriuchishima, T., Horaguchi, T., Morimoto, Y. et al. Intensity of physiotherapy after anterior cruciate ligament reconstruction: a comparison of two rehabilitation regimen. Arch Orthop Trauma Surg 130, 1053–1058 (2010). https://doi.org/10.1007/s00402-010-1134-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-010-1134-z