
Abstract
Introduction
Occult fractures of the proximal femur are not evident on radiographs and the diagnoses are often missed or delayed. We tried to determine whether the delay of diagnosis in elderly patients lead to increased morbidity and increased need for operation.
Materials and methods
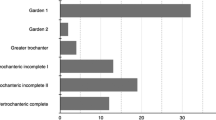
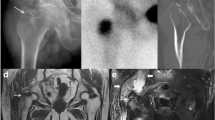
We identified 26 elderly patients (≥65 years of age) who were diagnosed as having an occult fracture of the proximal femur over a 3-year period. In 17 patients (17 hips, non-delayed group), the occult fracture was suspected at the first visit and the diagnosis was made on CT and/or MR images (MRI). In the remaining nine patients (9 hips, 34.6% delayed group), the diagnosis was delayed by a mean of 8.4 days (range 4–25 days). We compared the occurrence of fracture displacement, need for operation, change in activity level, and mortality between the non-delayed and delayed groups.
Result
Displacement of fracture occurred in 4 of 9 delayed patients and none of 17 non-delayed patients. Ten non-delayed patients needed operative treatment, whereas eight delayed patients needed operative treatment (p = 0.190). The activity level decreased in 6 of 7 surviving patients of the delayed group, whereas it decreased in 4 of 15 surviving patients of the non-delayed group (p = 0.020).
Conclusion
A delayed diagnosis of occult fracture in elderly patients resulted in increased rate of secondary displacement of the fracture and increased morbidity. In patients suspected of having occult hip fractures, additional studies, such as MRI and/or CT scans should be recommended to confirm the presence of hip fracture.



Similar content being viewed by others

References
Ray NF, Chan JK, Thamer M, Melton LJ 3rd (1997) Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res 12:24–35
Melton LJ 3rd (1993) Hip fractures: a worldwide problem today and tomorrow. Bone 14S:1–8
Randell A, Sambrook PN, Nguyen TV et al (1995) Direct clinical and welfare costs of osteoporotic fractures in elderly men and women. Osteoporos Int 5:427–432
Lubovsky O, Liebergall M, Mattan Y, Weil Y, Mosheiff R (2005) Early diagnosis of occult hip fractures MRI versus CT scan. Injury 36:788–792
Helland EB, Tollefsen I, Reksten G (2000) Radiographic diagnosis of the occult hip fracture: experience in 16 patients. Acta Orthop Scand 71:639–641
Verbeeten KM, Hermann KL, Hasselqvist M et al (2005) The advantages of MRI in the detection of occult hip fractures. Eur Radiol 15:165–169
Moore MN (1988) Orthopedic pitfalls in emergency medicine. South Med J 81:371–378
Bentley G (1980) Treatment of nondisplaced fractures of the femoral neck. Clin Orthop Relat Res 152:93–101
Mullen JO, Mullen NL (1992) Hip fracture mortality. A prospective, multifactorial study to predict and minimize death risk. Clin Orthop Relat Res 280:214–222
Murcia M, Brennan RE, Edeiken J (1982) Computed tomography of stress fracture. Skeletal Radiol 8:193–195
Tidermark J, Zethraeus N, Svensson O, Törnkvist H, Ponzer S (2002) Quality of life related to fracture displacement among elderly patients with femoral neck fractures treated with internal fixation. J Orthop Trauma 16:34–38
Blickenstaff LD, Morris JM (1996) Fatigue fracture of the femoral neck. J Bone Joint Surg Am 48:1031–1047
Zuckerman JD, Skovron ML, Koval KJ, Aharonoff G, Frankel VH (1995) Postoperative complications and mortality associated with operative delay in older patients who have a fracture of the hip. J Bone Joint Surg Am 77:1551–1556
Rizzo PF, Gould ES, Lyden JP, Asnis SE (1993) Diagnosis of occult fractures about the hip. Magnetic resonance imaging compared with bone-scanning. J Bone Joint Surg Am 75:395–401
Parker MJ (1992) Missed hip fractures. Arch Emerg Med 9:23–27
Hossain M, Barwick C, Sinha AK, Andrew JG (2007) Is magnetic resonance imaging (MRI) necessary to exclude occult hip fracture? Injury 38:1204–1208
Dominguez S, Liu P, Roberts C, Mandell M, Richman PB (2005) Prevalence of traumatic hip and pelvic fractures in patients with suspected hip fracture and negative initial standard radiographs—a study of emergency department patients. Acad Emerg Med 12:366–369
Sankey RA, Turner J, Lee J, Healy J, Gibbons CE (2009) The use of MRI to detect occult fractures of the proximal femur: a study of 102 consecutive cases over a ten-year period. J Bone Joint Surg Br 91:1064–1068
Hayes CW, Balkissoon AR (1997) Current concepts in imaging of the pelvis and hip. Orthop Clin North Am 28:617–642
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, KC., Ha, YC., Kim, TY. et al. Initially missed occult fractures of the proximal femur in elderly patients: implications for need of operation and their morbidity. Arch Orthop Trauma Surg 130, 915–920 (2010). https://doi.org/10.1007/s00402-010-1105-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-010-1105-4