
Abstract
Introduction
Tuberculosis arthritis of the hip is a crippling disease and there is need for an effective and acceptable treatment for the hips with bone destruction. The aim of this report was to evaluate the efficacy of the diagnostic method for hip tuberculosis and clinical results of the patients to clarify the question of whether a total hip arthroplasty (THA) should be attempted on a patient with a current or previous infection.
Materials and methods
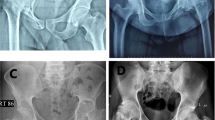
Nine patients with active tuberculosis of the hip, treated by cementless THA, were analyzed retrospectively. The mean age of the patients at diagnosis was 43.4 years (range 22–72 years). Laboratory tests of all the patients revealed high erthrocyte sedimentation rates (ESR) and C-reactive proteins. Plain radiographs showed bone destruction with joint space narrowing in all patients. Magnetic resonance imaging (MRI) scans showed fluid within the joint in five patients. Two patients had associated pulmonary tuberculosis. To confirm the clinico-radiological diagnosis, an open biopsy was performed for histopathological examinations of all the hips. Tuberculosis of the hips was treated with primary cementless THA, followed by postoperative antituberculous medication for 1 year. The inflamed soft tissues and the destroyed bones were completely resected and curetted out at the time of operation.
Results
At the final evaluation, the mean Harris Hip Score improved to 94.8 (range 90–98; P = 0.003). ESR became normal, less than 15 mm/h, with a mean time of 4 months (range 2–9 months). The C-reactive protein was normal, less than 0.8 mg/dl, after a mean time of 3 months (range 1–7 months). With an average follow-up of 5.6 years (range 2–8 years), no reactivation of tuberculosis infection was found in each patient. All of the femoral stems and acetabular cups were radiologically stable and demonstrated signs of bone ingrowth at the final follow-up. All histopathologic examinations showed granulomatous lesions including epitheloid histiocytes surrounded by lymphocytes.
Conclusions
Cementless THA can be safely performed in advanced tuberculosis of the hip for providing symptomatic relief and functional improvement of the hips. Complete curettage and resection of the infected tissue and postoperative antituberculous chemotherapy with a minimum of 1-year duration are very important in preventing reactivations.



Similar content being viewed by others


References
Asitava M (1994) Cytological diagnosis of vertebral tuberculosis with fine-needle aspiration biopsy. J Bone Joint Surg Am 76:181–184
Babhulkar S, Pande S (2002) Extraspinal tuberculosis: tuberculosis of the hip. Clin Orthop 398:93–99
Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr (1973) Ectopic ossification following total hip replacement: incidence and a method of classification. J Bone Joint Surg Am 55:1629–1632
Campbell JAB, Hoffman EB (1995) Tuberculosis of the hip in children. J Bone Joint Surg Br 77:319–326
Caparros AB, Sousa M, Zabalbeascou JR, Carrascosa PV, Corral FM (1999) Total hip arthroplasty for tuberculous coxitis. Int Orthop 23:348–350
Engh CA, Bobyn JD, Glassman AH (1987) Porous-coated hip replacement: the factors governing bone ingrowth, stress shielding and clinical results. J Bone Joint Surg Br 69:45–49
Eskola A, Santavita S, Kattinen YT, Tallroth K, Hoikka V, Lindholm ST (1998) Cementless total replacement for old tuberculosis of the hip. J Bone Joint Surg Br 70:603–606
Griffith JF, Kumta SM, Leung PC, Cheng JCY, Chow LTC, Metreweli C (2002) Imaging of musculoskeletal tuberculosis: a new look at an old disesase. Clin Orthop 398:32–39
Hardinge K, Cleary J, Charnley J (1979) Low-friction arthroplasty for healed septic and tuberculous arthritis. J Bone Joint Surg Br 61:144–147
Harris WH (1969) Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty: an end-result study using a new method of result evaluation. J Bone Joint Surg Am 51:737–755
Horan FT (2005) Historical notes: Robert Jones, Gathorne Girdlestone and excision arthroplasty of the hip. J Bone Joint Surg Br 87:104–106
Hugate R, Pellegrini V (2002) Reactivation of ancient tuberculous arthritis of the hip following total hip arthroplasty: a case report. J Bone Joint Surg Am 84:101–105
Ihora K, Toyoda K, Ofuji A, Kawai S (1998) Tuberculous bursitis of the greater trochanter. J Orthop Sci 3:120–124
Jain AK, Jena SK, Singh MP, Dhamni IK, Ramachadran VG, Dev G (2008) Evaluation of clinico-radiological, bacteriological, serological, molecular and histological diagnosis of osteoarticular tuberculosis. Indian J Orthop 42:173–177
Joshi AB, Markovic L, Hardinge K, Murphey CY (2002) Conversion of a fused hip to total hip arthroplasty. J Bone Joint Surg Am 84:1335–1341
Jupiter JB, Karchmer AW, Lowell JD, Harris WH (1981) Total hip arthroplasty in the treatment of adult hips with current or quiescent sepsis. J Bone Joint Surg Am 63:194–200
Kaya M, Nagoya S, Yamashito T, Niiro N, Fujita M (2005) Periprosthetic tuberculosis infection of the hip in a patient with no previous history of tuberculosis. J Bone Joint Surg Br 88:394–395
Kim YH, Han DY, Park BM (1987) Total hip arthroplasty for tuberculous coxarthrosis. J Bone Joint Surg Am 69:718–727
Kim YY, Ahn BH, Bae DK, Ko CV, Lee JD, Kwak BM, Yoon YS (1986) Arthroplasty using the Charnley prosthesis in old tuberculosis of the hip: clinical experience with 8–10 year follow-up evaluation. Clin Orthop 211:116–121
Kim YY, Ahn JY, Shim JC, Park HS, Bai GH (2001) Long-term results of Charnley low-friction arthroplasty in tuberculosis of the hip. J Arthroplasty 16(Suppl 1):S106–S110
Kim YY, Kim BJ, Ko HS, Sung YB, Kim SK, Shim JC (1998) Total hip reconstruction in the anatomically distorted hip: cemented versus hybrid total hip arthroplasty. Arch Orthop Trauma Surg 117:8–14
Kim YH, Oh SH, Kim JS (2003) Total hip arthroplasty in adult patients who had childhood infection of the hip. J Bone Joint Surg Am 85:198–204
Krappel FA, Harland U (2000) Failure of osteosynthesis and prosthetic joint infection due to Mycobacterium tuberculosis following a subtrochanteric fracture: a case report and review of the literature. Arch Orthop Trauma Surg 120:470–472
Langley GB, Sheppeard H (1985) The visual analogue scale: its use in pain measurement. Rheumatol Int 5:145–148
Shembekar A, Babhulkar S (2002) Chemotherapy for osteoarticular tuberculosis. Clin Orthop 398:20–26
Shen HL, Xia Y, Li P, Wang J, Han H (2009) Arthroscopic operations in knee joint with early-stage tuberculosis. Arch Orthop Trauma Surg. doi:10.1007/s00402-009-0881-1
Tuli SM (2002) General principles of osteoarticular tuberculosis. Clin Orthop 398:11–19
Watts H, Lifeso R (1996) Tuberculosis of bones and joints. J Bone Joint Surg Am 78:288–299
Yoon TR, Rowe SM, Anwar IB, Chung JY (2001) Active tuberculosis of the hip treated with early total hip replacement: a report of 3 cases. Acta Orthop Scand 72:419–421
Yoon TR, Rowe SM, Santosa SB, Jung ST, Seon JK (2005) Immediate cementless total hip arthroplasty for the treatment of active tuberculosis. J Arthroplasty 20:923–926
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Öztürkmen, Y., Karamehmetoğlu, M., Leblebici, C. et al. Cementless total hip arthroplasty for the management of tuberculosis coxitis. Arch Orthop Trauma Surg 130, 197–203 (2010). https://doi.org/10.1007/s00402-009-0967-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-009-0967-9