
Abstract
Purpose
Despite high accuracy of magnetic resonance imaging (MRI) for diagnosing meniscal tears, MR findings do not always agree with surgical findings. We performed a blinded, retrospective study to analyze the nature and frequency of errors in the MR diagnosis of meniscal tears.
Materials and methods
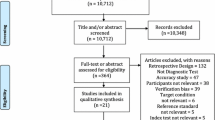
Medical records of 100 consecutive patients who underwent MR and arthroscopy of the knee at our institution were reviewed. Twelve patients underwent prior meniscal surgery. Twenty-three patients had 27 discrepancies between MR and surgical findings. These were independently reviewed by two additional musculoskeletal radiologists in a double blinded fashion. Original incorrect diagnoses were categorized as either unavoidable, interpretation error or equivocal for meniscal tear.
Results
MR accuracy was 88% for the medial and 85% for the lateral meniscus. Of 27 incorrect MR diagnoses, 12 (44%) were unavoidable, 10 (37%) equivocal and 5 (19%) interpretation errors. Of the 67 medial meniscal tears, 12 (18%) were missed. Eight (67%) of these 12 were categorized as equivocal, including three postoperative menisci. Of 30 lateral tears, 12 (40%) were missed, 7 (58%) of which were categorized as unavoidable. Of these 12, 11 (92%) showed fraying of the inner edge, which was shaved at arthroscopy (n = 8) or had stable tear treated conservatively (n = 3). There were three false-positive diagnoses, all occuring in the lateral meniscus, two of which were unavoidable and one interpretation error.
Conclusion
Of all missed lateral meniscal tears, most are unavoidable and related to confusion between what represents fraying and what represents a tear. Unavoidable false-positive diagnoses are infrequent and may be related to incomplete arthroscopic evaluation. Subtle or equivocal findings still make MR diagnosis difficult, even for experienced radiologists.




Similar content being viewed by others


References
Elvenes J, Jerome CP, Reikeräs, Johansen O (2000) Magnetic resonance imaging as a screening procedure to avoid arthroscopy for meniscal tears. Arch Orthop Trauma Surg 120:14–16
Sanders TG, Miller MD (2005) A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries to the knee. Am J Sports Med 33:131–148
De Smet AA, Tuite MJ, Norris MA, Swan JS (1994) MR diagnosis of meniscal tears: analysis of causes of errors. AJR 163:1419–1423
Justice WW, Quinn SF (1995) Error patterns in the MR Imaging evaluation of menisci of the knee. Radiology 196:617–621
Quinn SF, Brown TF (1991) Meniscal tears diagnosed with MR imaging versus arthroscopy: how reliable is a standard arthroscopy?. Radiology 181:843–847
Deutsch AL, Mink JH, Fox JM et al (1990) Peripheral meniscal tears: MR findings after conservative treatment or arthroscopic repair. Radiology 176:485–488
De Smet AA, Norris MA, Yandow DR, Graf BK, Keene JS (1993) Diagnosis of meniscal tears of the knee with MR imaging: effect of observer variation and sample size on sensitivity and specificity. AJR 160:555–559
Sproule JA, Khan F, Rice JJ, Nicholson P, McElwain JP (2005) Altered signal intensity in the posterior horn of the medial meniscus: an MR finding of questionable significance. Arch Orthop Trauma Surg 125:267–271
De Smet AA, Norris MA, Yandow DR, Quintana FA, Graf BK, Keene JS (1993) MR diagnosis of meniscal tears of the knee: importance of high signal in the meniscus that extends to the surface. AJR 161:101–107
Anderson MW (2002) MR imaging of the meniscus. Radiol Clin North Am 40:1081–1094
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Van Dyck, P., Gielen, J., D’Anvers, J. et al. MR diagnosis of meniscal tears of the knee: analysis of error patterns. Arch Orthop Trauma Surg 127, 849–854 (2007). https://doi.org/10.1007/s00402-007-0318-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-007-0318-7