
Abstract
Introduction
Charcot-neuro-osteoarthropathy with its severe destruction of bones remains a challenge for physicians and surgeons. The aim of the study was to characterise a patient population treated in a specialised foot care centre who underwent surgical treatment for their diabetic foot syndrome. Special attention was paid to patients who suffered from Charcot-neuro-osteoarthropathy and the impact of Syme amputation if amputation of the foot was inevitable.
Materials and methods
A total of 121 patients with diabetic foot syndrome and ulcerations underwent an interdisciplinary strategy for diagnostic and therapeutic procedures including MRI and surgical interventions. If peripheral arterial vessel disease was present, revascularisation by distal bypass grafting was done before the orthopaedic intervention. Some 24% showed the typical neuro-osteoarthropathy with severe bone destruction. In 8 cases amputation of the foot was performed using the Syme technique.
Results
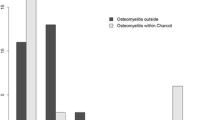
In our population the short-term results (follow-up 12 months, 20% lost to follow-up) are good, only 4% of the patients required further surgery on the same foot. In all patients with Charcot feet, plain radiographs showed the typical radiographic signs of the disease, and MRI was most helpful to detect abscess formations. The typical clinical problems of patients with Charcot disease are pointed out, and conservative and surgical treatment options are discussed. All patients with Syme amputation did well, wound healing and weight-bearing of the limb were accomplished.
Conclusion
The crucial diagnostic tool for decision-making in diabetic foot syndrome was MRI, which normally shows osteomyelitis with high sensitivity and specificity. In patients with Charcot-neuro-osteoarthropathy, the bone marrow oedema of the involved parts of the skeleton might misleadingly suggest the diagnosis of osteomyelitis. If amputation is inevitable in severe abscess formation combined with instability and perforation of the dislocated and destroyed bones in Charcot-neuro-osteoarthropathy, these patients might benefit from a foot amputation according to the technique Syme described. For this procedure the blood supply of the posterior tibial artery is essential. All these patients were able to walk without support. The material presented helps to generate hypotheses for further prospective studies.





Similar content being viewed by others

References
Baumgartner G (1999) Chirurgisches Vorgehen bei Neuropathie und Osteoarthropathie des Diabetischen Fußes. Zentralbl Chir 124:17–24
Brower AC, Allman RM (1981) Pathogenesis of the neurotrophic joint: neurotraumatic vs. neurovasular. Radiology 139:349–354
Cavanagh PR, Young MJ, Adams JE, Vickers KL, Boulton AJM (1994) Radiographic abnormalities in the feet of patients with diabetic neuropathy. Diabetes Care 17:201–109
Charcot JM, Féré C (1883) Affections osseuses et articulaires du pied chez les tabétiques (pied tabétique). Progrès Médical SI: 606–607
Cofield RH, Morrison MJ, Beabout JW (1983) Diabetic neuroarthropathy in the foot: patient characteristics and patterns of radiographic change. Foot Ankle 4:15–22
Eichenholtz SN (1966) Charcot joints. Charles C.Thomas, Springfield
Fortin PT (2001) The diabetic foot. Basic concepts – the Charcot foot. Instructional Course lectures 181, AAOS
Gough A, Abraha H, Li F, Purewal TS, Foster AVM, Watkins PJ, Moniz C, Edmonts ME (1997) Measurement of markers of osteoclast and osteoblast activity in patients with acute and chronic diabetic Charcot neuroarhropathy. Diabet Med 14:527–531
Griffiths HJ (1985) Diabetic osteopathy. Orthopedics 8:401–406
Guyton GP (2001) The diabetic foot – the basics: epidemiology, pathophysiology, and pharmacology. Instructional Course Lectures 181, AAOS
Hammerl B, Haller J, Keck AV, Pecherstorfer M (2000) Oral alendronate for treatment of Charcot neuroosteoarthropathy. Osteologie 9:129–132
Johnson JTH (1967) Neuropathic fractures and joint injuries. Pathogenesis and rationale of prevention and treatment. J Bone Joint Surg Am 49:1–30
Johnson JE (1998) Operative treatment of neuropathic arthropahy of the foot and ankle. J Bone Joint Surg Am 80:1700–1709
Larsson J, Agardt CD, Apelqvist J, Stenström A (1998) Long-term prognosis after healed amputation in patients with diabetes. Clin Orthop 350:149–158
Onvlee GJ (1998) The Charcot foot. A critical review and an observational study of a group of 60 patients. Dissertation, University of Leiden
Pinzur MS (1999) Restoration of walking ability with Syme’s ankle disarticulation. Clin Orthop 361:71–75
Sanders LJ, Frykberg RG (1991) Diabetic neuropathic osteoarthropathy: the Charcot foot. In: Frykberg RG (ed) The high risk foot in diabetes mellitus. Churchill Livingstone, New York, pp 297–338
Schon LC, Easley ME, Weinfeld SB (1998) Charcot neuroarhropathy of the foot and ankle. Clin Orthop 349:116–131
Schoonheid PH (1884) Die Resultate der chirurgischen Behandlung neuropathischer Gelenkaffektionen. Dissertation, University of Heidelberg
Wetz HH, Baumgartner G (1998) Die orthopädisch-chirurgische Behandlung der diabetisch-neuropathischen Osteoarthropathie. Med Orthop Tech 118:6-14
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Eckardt, A., Schöllner, C., Decking, J. et al. The impact of Syme amputation in surgical treatment of patients with diabetic foot syndrome and Charcot-neuro-osteoarthropathy. Arch Orthop Trauma Surg 124, 145–150 (2004). https://doi.org/10.1007/s00402-003-0622-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-003-0622-9