
Abstract
Introduction
In this study, the results of ulnar nerve repair were analyzed. The relation between the functional outcome scores and clinical findings were investigated to find out whether any clinical finding could be predictive of the outcome.
Materials and methods
Seventeen patients who underwent ulnar nerve repair formed the study group. Average follow-up lasted 45.5 months (range 39–48 months), and average age of the study group was 31.7 years (range 26–42 years). The same operative technique was applied to all patients by one of the authors (HG). Follow-up checks were done at 3, 6, and 12 months postoperatively. The patients who did not attend the last follow-up were excluded from the study group. The Seddon classification was used as the functional scoring system. Wound healing, Tinel sign, interosseous atrophy, atrophy of the first web space, clawing, and protective sensation were the clinical findings examined at the follow-ups. Wound healing was classified as either normal scar formation or hypertrophic scar-keloid (HsC) formation.
Results
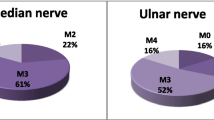
Good results in 4 and fair results in 13 were obtained according to the Seddon classification. Statistically, there was no difference between the clinical findings at the 3, 6, and 12 month follow-ups.
Conclusion
Presence of HsC and clawing can be regarded as a predictive sign for fair results in nerve repairs.
Similar content being viewed by others


References
Bolesta MJ, Garret WE, Ribbeck BM, Glisson RR, Seaber AV, Goldner L (1988) Immediate and delayed neuroraphy in a rabbit model: a functional, histologic, and biomechanical comparison. J Hand Surg Am 13:364–369
Brich R, Raji AR (1991) Repair of median and ulnar nerves. Primary suture is best. J Bone Joint Surg Br 73:154–157
Chvapil M, Koopmann CF (1984) Scar formation: physiology and pathological states. Otolaryngologic Clin North Am 17:265–272
Deutinger M, Girsch W, Burggasser G, Vinisch A, Matry N, Freilinger G (1993) Clinical and electroneurographic evaluation of sensory/motor-differentiated nerve repair in the hand. J Neurosurg 78:709–713
Hentz VR, Rosen JM, Wiao S-J, McGill KC, Abraham G, Alto P (1993) The nerve gap dilemma: a comparison of nerves repaired end to end under tension with nerve grafts in a primate model. J Hand Surg Am 18:417–425
Hudson DA, Jager LT (1993) The spaghetti wrist. J Hand Surg Br 18:171–173
Kim DH, Connolly SE, Gillespie JT, Voorries RM, Kline DG (1991) Electrophysiological of various graft and lesion lengths in repair of nerve gaps in primates. J Neurosurg 75:440–446
Lundborg BR, Dahlin LB, Karlson B (1994) Nerve repair: correlation of restitution of functional sensibility with specific cognitive capacities. J Hand Surg Br 19:452–458
Lundborg G, Rosen B (2001) Sensory relearning after nerve repair. Lancet 358:809–810
Mackinnon SE, Dellon AL (1988) Diagnosis of nerve injury. In: Mackinnon SE, Dellon AL (eds) Surgery of the peripheral nerve. Thieme Medical Publishers, New York, pp 65–88
Seddon HJ(1954) Nerves injuries committee of the British Medical Research Council. In: Seddon HJ (ed) Peripheral nerve injuries. MRC special report series. Her Majesty’s Stationery Office, London, no. 282, pp 10–11
Smith JW (1996) Factors influencing nerve repair. Arch Surg 93:335–341
Tredget EE, Nedelec B, Scott PG, Ghalary A (1997) Hypertrophic scars, keloid, and contractures. The cellular and molecular basis for therapy. Surg Clin North Am 77:701–730
Witte MB, Barbul A (1997) General principles of wound healing. Surg Clin North Am 77:509–528
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gurbuz, H., Aktas, S. & Calpur, O.U. Clinical evaluation of ulnar nerve repair at wrist level. Arch Orthop Trauma Surg 124, 49–51 (2004). https://doi.org/10.1007/s00402-003-0587-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-003-0587-8