
Abstract
Aim
The need for implantable cardioverter-defibrillator (ICD) defibrillation testing (DT) and subsequent intraoperative system modifications is discussed controversially. The study’s goal was to prove that consequent abdication of intraoperative DT does not impair defibrillation efficacy and does not increase the rate of postoperative system revisions.
Methods
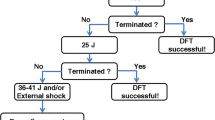
In a prospective single-center observational study, 609 out of 648 consecutive patients underwent transvenous ICD implantation (left-sided, active can, dual coil lead, and biphasic shock waveform) waiving intraoperative DT. Defibrillation efficacy was validated prior to hospital discharge (PHD) by applying two 10 J safety margin (SM) shocks.
Results
Following “schockless” implantation 580 out of 609 patients (95.2 %) met a 10 J SM with default programming. Shock path reversal provided 10 J SM in 13 out of 29 cases with initially failed DT. In four patients (0.7 %) maximum energy shocks were ineffective. There was no morbidity or mortality related to DT. The total rate of surgical ICD revisions was 1.8 %.
Conclusion
Routine ICD implantation without intraoperative DT does not lead to an increased rate of postoperative system modifications and does not decrease defibrillation efficacy as tested PHD.
Zusammenfassung
Hintergrund
Der Nutzen der intraoperativen ICD-Testung sowie resultierender Systemmodifikationen wird nach wie vor kontrovers diskutiert. Ziel der Studie war es nachzuweisen, dass der Verzicht auf eine intraoperative Routine-Testung in einem konsekutiven Patientengut 1) die Defibrillationseffektivität nicht beeinträchtigt und 2) nicht zu einer Erhöhung der Rate postoperativer Revisionen führt.
Patienten und Methoden
In der prospektiven monozentrischen Beobachtungsstudie wurde bei 609 aus 648 konsekutiven Patienten ein transvenöser 1- oder 2-Kammer-ICD (links pectoral, active can, dual-coil-Elektrode, biphasische Schocks) konsequent ohne intraoperative Testung implantiert. Die Defibrillationseffektivität wurde vor stationärer Entlassung mittels Testung der 10 Joule Sicherheitsmarge überprüft.
Ergebnisse
In der Standardkonfiguration ließ sich bei 580 von 609 Patienten (95,2 %) eine 10 J Sicherheitsmarge nachweisen. Bei 13 der 29 Patienten mit initial negativem Test wurde nach Umkehr des Schockpfades eine adäquate Sicherheitsmage dokumentiert. In 4 Fällen (0,7 %) waren Schocks mit maximaler Energie ineffektiv. Die Gesamtrate notwendiger chirurgischer Revisionen lag bei lediglich 1,8 %.
Schlußfolgerung
Der Verzicht auf eine intraoperative Testung führte in einem unselektionierten Kollektiv von ICD-Patienten nicht zu einer Reduktion der vor stationärer Entlassung überprüften Defibrillationseffektiviät und erhöhte nicht die Rate notwendiger Systemmodifikationen.

Similar content being viewed by others
References
Bianci S, Ricci RP, Biscione F, Sgreccia F, Di BN, Rossi P et al (2009) Primary prevention implantation of cardioverter defibrillator without defibrillation threshold testing: 2-year follow-up. Pacing Clin Electrophysiol 32:573–578
Blatt JA, Poole JE, Johnson GW, Callans DJ, Raitt MH, Reddy RK et al (2008) No benefit from defibrillation threshold testing in the SCD-HeFT (sudden cardiac death in Heart Failure Trial). J Am Coll Cardiol 52:551–556
Brignole M, Raciti G, Bongiorni MG, De Martino G, Favale S, Gasparini M et al (2007) Defibrillation testing at the time of implantation of cardioverter defibrillator in the clinical practice: a nation-wide survey. Europace 9:540–543
Brunn J, Böcker D, Weber M, Castrucci M, Gradaus R, Borggrefe M et al (2000) Is there a need for routine testing of ICD defibrillation capacity? Eur Heart J 21:162–169
Calvi V, Dugo D, Capodanno D, Arancio R, Di GA, Liotta C et al (2010) Intraoperative defibrillation threshold testing during implantable cardioverter-defibrillator insertion: do we really need it? Am Heart J 159:98–102
Christ G, Becker R, Voss F, Kelemen K, Senges-Becker J, Hauck M et al (2007) Indications for predismissal testing with arrhythmia-induction in patients receiving an implantable cardioverter defibrillator. Clin Res Cardiol 96:613–620
Duray GZ, Hohnloser SH (2010) Defibrillation testing: the need for a definitive trial. J Cardiovasc Electrophysiol 21:183–185
Fisher JD (2011) Defibrillation testing: philosophy and science. Pacing Clin Electrophysiol 34:185
Gasparini M, Galimberti P, Regoli F, Ceriotti C, Bonadies M (2005) Delayed defibrillation testing in patients implanted with biventricular ICD (CRT-D): a reliable and safe approach. J Cardiovasc Electrophysiol 16:1279–1283
Gold MR, Kroll MW, Ellenbogen KA (2009) Defibrillation testing at ICD implantation: are we asking the wrong question? Pacing Clin Electrophysiol 32:567–569
Gula LJ, Massel D, Krahn AD, Yee R, Skanes AC, Klein GJ (2008) Is defibrillation testing still necessary? A decision analysis and Markov Model. J Cardiovasc Electrophysiol 19:400–405
Hall B, Jeevanantham V, Levine E, Daubert J, McNitt S, Morady F, Pelosi F (2007) Comparison of outcomes in patients undergoing defibrillation threshold testing at the time of implantable cardioverter-defibrillator implantation versus no defibrillation threshold testing. Cardiol J 14:463–469
Healey JS, Dorian P, Mitchell LB, Talajic M, Philippon F, Simpson C, Yee R et al (2010) Canadian Registry of ICD Implant Testing Procedures (CREDIT): current practice, risks, and costs of intraoperative defibrillation testing. J Cardiovasc Electrophysiol 21:177–182
Kolb C, Tzeis S, Zrenner B (2009) Defibrillation threshold testing: tradition or necessity? Pacing Clin Electrophysiol 32:570–572
DeSouza CM, Koehler JL, DeGroot PJ (1998) Failing defibrillator implant criterion on the initial attempt is a predictive factor for sudden cardiac death. Pacing Clin Electrophysiol 21:801
Mewis C, Neuberger HR, Buob A (2010) Is intraoperative ICD-testing still necessary? Herzschr Elektrophys 21:123–128
Neuzner J (2005) Is DFT testing still mandatory? Herz 30:601–606
Pires LA (2007) Defibrillation testing of the implantable cardioverter defibrillator: when, how, and by whom? Indian Pacing Electrophysiol J 7(3):166–175
Pires LA, Johnson KM (2006) Intraoperative testing of the implantable cardioverter-defibrillator: how much is enough? J Cardiovasc Electrophysiol 17:140–145
Russo AM, Sauer W, Gerstenfeld EP, Hsia HH, Lin D, Cooper JM et al (2005) Defibrillation threshold testing: is it really necessary at the time of implantable cardioverter-defibrillator insertion? Heart Rhythm 2:456–461
Strickberger SA, Klein GJ (2004) Is defibrillation testing required for defibrillator implantation? J Am Coll Cardiol 44:88–91
Swerdlow ChD, Russo AM, Degroot PJ (2007) The dilemma of ICD implant testing. Pacing Clin Electrophysiol 30:675–700
Theuns DAMJ, Szili-Torok T, Jordaens LJ (2005) Defibrillation efficacy testing: long-term follow-up and mortality. Europace 7:509–515
Viskin S, Rosso R (2008) The top 10 reasons to avoid defibrillation threshold testing during ICD implantation. Heart Rhythm 5(3):391–393
Vlay SC (2009) Defibrillation threshold testing in the 21st century: necessary or Not? Pacing Clin Electrophysiol 32:565–566
Weiss DN, Zilo P, Luceri RM, Platt S, Rosenbaum M (1997) Predischarge arrhythmia induction testing of implantable defibrillators may be unnecessary in selected cases. Am J Cardiol 80:1562–1565
Sweidan R, Pokushalov E, Kuznetsov V, Kubíčková M, Bastian D, Naik A et al (2010) Defibrillation testing in different ICD-subpopulations: Results from PANORAMA. Europace 12(S1):i90
Uyguanco ER, Berger A, Budzikowski AS, Gunsburg M, Kassotis J (2008) Management of high defibrillation threshold. Expert Rev Cardiovasc Ther 6(9):1237–1248
Degroot PJ, Church TR, Mehra R, Martinson MS, Schaber DE (1997) Derivation of a defibrillator implant criterion based on probability of successful defibrillation. Pacing Clin Electrophysiol 20:1924–1935
DeGroot PJ, DeSouza CM, Wang WX (1999) Is testing defibrillation efficacy during defibrillator implant worth it? Pacing Clin Electrophysiol 22:723
Barold SS, Herweg B, Curtis AB (2005) the defibrillation safety margin of patients receiving ICDS: a matter of definition. Pacing Clin Electrophysiol 28:881–882
Schauerte P, Stellbrink C, Schöndube FA, Löser H, Haltern G, Messmer BJ, Hanrath P (1997) Polarity reversal improves defibrillation efficacy in patients undergoing transvenous cardioverter defibrillator implantation with biphasic shocks. Pacing Clin Electrophysiol 20(Pt 1):301–306
Gold MR, Higgins S, Klein R, Gilliam FR, Kopelman H, Hessen S et al (2002) Efficacy and temporal stability of reduced safety margins for ventricular defibrillation. Primary results from the Low Energy Safety Study (LESS). Circulation 105:2043–2048
Toal SC, Harris L, Asta J, Hill A, Cameron DA (2006) Routine defibrillation threshold testing at implant in patients receiving defibrillators for primary prevention: is this necessary? Heart rhythm 3:157
Shukla HH, Flaker GC, Jayam V, Roberts D (2003) High defibrillation thresholds in transvenous biphasic implantable defibrillators: clinical predictors and prognostic implications. Pacing Clin Electrophysiol 26(Pt 1):44–48
Buob A, Siaplaouras S, Tscholl D, Schäfers H-J, Böhm M, Jung J (2004) Clinical value of routine predischarge testing after ICD-implantation. Europace 6:159–164
Delvecchio A, Trivedi HA, Fisher JD, Kim SG, Ferrick KJ, Gross JN, Palma EC (2005) Value of pre-hospital discharge defibrillation testing in recipients of implanted cardioverter defibrillators. Pacing Clin Electrophysiol 28:260–262
Val-Mejias JE, Oza A (2010) Does defibrillation threshold increase as left ventricular ejection fraction decreases? Europace 12:385–388
Sauer WH, Lowery CM, Bargas RL, Schuller JL, Stees CS, Aleong RG, Varosy PD (2011) Utility of postoperative testing of implantable cardioverter-defibrillators. Pacing Clin Electrophysiol 34:186–192
Alter P, Waldhans S, Plachta E, Moosdorf R, Grimm W (2005) Complications of implantable cardioverter defibrillator therapy in 440 consecutive patients. Pacing Clin Electrophysiol 28:926–932
Singer I, van derLJ, Edmonds HL Jr, Slater AD, Austin E, Shields CB, Kupersmith J (1991) Is defibrillation testing safe? Pacing Clin Electrophysiol 14(Pt 2):1899–1904
Birnie D, Tung S, Simpson C, Crystal E, Exner D, Paredes F-AA et al (2008) Complications associated with defibrillation threshold testing: the Canadian experience. Heart Rhythm 5:387–390
Roberts PR, Allen S, Betts T, Morgan JM, Urban JF, Whitman T et al (2000) Increased defibrillation threshold with right-sided active pectoral can. J Interv Card Electrophysiol 4(1):245–249
Mouchawar GA, Wolsleger WK, Doan PD, Causey JD 3rd, Kroll MW (1997) Does an SVC electrode further reduce DFT in a hot-can ICD system? Pacing Clin Electrophysiol 20(Pt 2):163–167
Rinaldi CA, Simon RDB, Geelen P, Reek S, Baszko A, Kuehl M, Gill JS (2003) A randomized prospective study of single coil versus dual coil defibrillation in patients with ventricular arrhythmias undergoing implantable cardioverter defibrillator therapy. Pacing Clin Electrophysiol 26:1684–1690
Gold M, Val-Mejias J, Leman RB, Tummala R, Goyal S, Kluger J et al (2008) Optimization of superior vena cava coil position and usage for transvenous defibrillation. Heart Rhythm 5:394–399
Gold MR, Olsovsky MR, Pelini MA et al (1998) A comparison of single and dual coil active pectoral defibrillation lead systems. J Am Coll Cardiol 31:1391–1394
Gasparini M, Galimberti P, Ceriotti C (2012) The values of defibrillation testing at implantable cardioverter defibrillator implantation: “and then there were none”. Curr Opin Cardiol 27(1):8–12
Michowitz Y, Lellouche N, Contractor T, Bourke T, Wiener I, Buch E et al (2011) Defibrillation threshold testing fails to show clinical benefit during long-term follow-up of patients undergoing cardiac resynchronization therapy defibrillator implantation. Europace 13(5):683–688
Conflict of interest and ethics.
All authors have seen and approved the paper. S. Kracker is Field Clinical Research Specialist of the Medtronic Bakken ResearchCenter, Maastricht, The Netherlands. D. Bastian received research grant from Medtronic, speaker fees from BSCI, Medtronic, SJM and serves as a consultant for Biotronik. M. Pauschinger and K. Göhl declare thatthere are no actual or potential conflicts of interest in relation to this article. The authors affirm that the manuscript is not under simultaneous consideration elsewhere and has not been previously published in similarform. The study complies with the Declaration of Helsinki.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bastian, D., Kracker, S., Pauschinger, M. et al. ICD implantation without intraoperative testing does not increase the rate of system modifications and does not impair defibrillation efficacy tested in follow-up. Herzschr Elektrophys 24, 125–130 (2013). https://doi.org/10.1007/s00399-013-0267-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00399-013-0267-5