
Abstract
Objectives
This study aims to estimate the impact of disease activity, obesity, functional disability, and depression on lipid status, glycoregulation, and risk for coronary heart disease (CHD) in patients with rheumatoid arthritis (RA).
Patients and methods
A total of 36 patients with RA (30 women and 6 men, mean age 54.9 years, mean disease duration 7.9 years) were included in this study. We estimated the impact of age, body mass index, disease activity [assessed by DAS28 index and C-reactive protein (CRP) value], functional ability (estimated using the HAQ disability index), and depression [assessed using the Beck Depression Inventory (BDI)] on glycoregulation, lipid status, and risk for CHD in our patients. Glycoregulation was assessed by measuring insulin resistance, insulin, and glucose in blood. Lipids tested in blood included total cholesterol, HDL and LDL cholesterol, and triglycerides (TG). The 10-year risk for CHD was estimated using the Framingham risk score.
Results
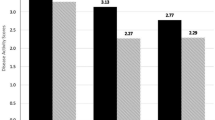
Of 36 patients, 11 (30.6 %) fulfilled the criteria for metabolic syndrome (MS). Ten of 11 patients (90.1 %) with MS have a 10-year risk for CHD greater than 10 % compared to only 3 of 25 patients (12 %) without MS (p = 0.0001). Patients with high disease activity had lower HDL values than patients with mild or moderate disease activity (1.4 vs. 1.7 mmol/l, p = 0.04). Significant correlations were observed between CRP level and insulinemia (ρ = 0.57, p = 0.003), as well as CRP level and the HOMA index (ρ = 0.59, p = 0.002). The body mass index (BMI) correlated significantly with total cholesterol (r = 0.46, p = 0.02), LDL (ρ = 0.41, p = 0.04), and TG (ρ = 0.65, p < 0.001) in blood. The HAQ-DI did not correlate either with parameters of glycoregulation or lipid status. There was a significant positive correlation between BDI and BMI (ρ = 0.60, p < 0.001).
Conculsion
Active RA is independently associated with decreased HDL cholesterol and increased insulin resistance. Obesity was found to be an independent risk factor for increased total cholesterol, LDL cholesterol, and TG. Depressed patients with RA tend to be overweight or obese and, therefore, have an unfavorable lipid profile.
Zusammenfassung
Zielsetzung
Ziel der Studie ist die Untersuchung möglicher Einflüsse von Krankheitsaktivität, Adipositas, funktioneller Behinderung und Depression auf den Lipidstatus, die Glukoseregulation und das Risiko für eine koronare Herzerkrankung (KHK) bei Patienten mit rheumatoider Arthritis (RA).
Patienten und Methoden
Insgesamt 38 RA-Patienten (30 weiblich, 6 männlich, Durchschnittsalter 54,9 Jahre, durchschnittliche Erkrankungsdauer 7,9 Jahre) wurden in die Studie aufgenommen. Abgeschätzt wurde der Einfluss von Alter, Body-Mass-Index, Erkrankungsaktivität [Assessment mittels DAS28-Index und CRP(C-reaktives Protein)-Konzentration], funktionalem Status (Näherung mittels HAQ Disability Index) und Depression [Messung mit dem BDI (Beck Depression Inventory)] auf die Glukoseregulation, den Lipidstatus und das KHK-Risiko. Laborchemisch bestimmt wurden Insulinresistenz, Insulin und Glukose sowie Gesamt-, HDL- und LDL-Cholesterin und Triglyzeride (TG). Das Zehnjahresrisiko für die Entwicklung einer KHK wurde anhand des Framingham-Risikoscores geschätzt.
Ergebnisse
Von 36 Patienten erfüllten 11 (30,6 %) Kriterien für das metabolische Syndrom (MS). Ein Zehnjahres-KHK-Risiko von über 10% haben 10 von 11 (90,1%) Patienten mit einem MS, dagegen nur 3 von 25 (12%) Patienten ohne MS (p = 0,0001). Patienten mit hoher Krankheitsaktivität hatten niedrigere HDL-Werte als Patienten mit geringer oder mäßiger Krankheitsaktivität (1,4 vs. 1,7 mmol/l, p = 0,04). Statistisch signifikante Korrelationen zeigten sich sowohl zwischen CRP-Werten und Insulinämie (ρ = 0,57, p = 0,003) als auch zwischen CRP und HOMA-Index (ρ = 0,59, p = 0,002). Der Body-Mass-Index (BMI) korrelierte signifikant mit dem Gesamt- (r = 0,46, p = 0,02) und mit dem LDL-Cholesterin (ρ = 0,41, p = 0,04) sowie mit TG (ρ = 0,65, p < 0,001) im Serum. Der HAQ-DI-Score wies keine Korrelation auf mit Glukohomöostaseparametern oder dem Lipidstatus auf. Zwischen BDI und BMI bestand eine signifikante positive Korrelation (ρ = 0,60, p < 0,001).
Schlussfolgerungen
Eine aktive RA ist unabhängig assoziiert mit erniedrigten HDL-Cholesterin-Werten und erhöhter Insulinresistenz. Adipositas erwies sich als ein unabhängiger Risikofaktor für höhere Konzentrationen von Gesamtcholesterin, LDL-Cholesterin und TG. Depressive RA-Patienten neigen zu Übergewicht bzw. Adipositas und weisen daher ein ungünstiges Lipidprofil auf.
Similar content being viewed by others


References
Mutru O, Laakso M, Isomaki H, Koota K (1989) Cardiovascular mortality in patients with rheumatoid arthritis. Cardiology 76:71–77
Myllykangas-Luosujarvi R, Aho K, Kautiainen H et al (1995) Cardiovascular mortality in women with rheumatoid arthritis. J Rheumatol 22:1065–1067
Kaplan MJ (2006) Cardiovascular disease in rheumatoid arthritis. Curr Opin Rheumatol 18:289–297
Chung CP, Oeser A, Solus JF et al (2008) Prevalence of the metabolic syndrome is increased in rheumatoid arthritis and is associated with coronary atherosclerosis. Atherosclerosis 196:756–763
Festa A, D’Agostino R Jr, Howard G et al (2000) Chronic subclinical inflammation as part of the insulin resistance syndrome: the Insulin Resistance Atherosclerosis Study (IRAS). Circulation 102:42–47
Kiortsis DN, Mavridis AK, Vasakos S et al (2005) Effects of infliximab treatment on insulin resistance in with rheumatoid arthritis and ankylosing spondylitis. Ann Rheum Dis 64:765–766
Nurmohamed MT (2007) Atherogenic lipid profiles and its management in patients with rheumatoid arthritis. Vasc Health Risk Manag 3:845–852
Barth J, Schumacher M, Herrmann-Lingen C (2004) Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med 66:802–813
Covic T, Cumming SR, Pallant JF et al (2012) Depression and anxiety in patients with rheumatoid arthritis: prevalence rates based on a comparison of the Depression, Anxiety and Stress Scale (DASS) and the hospital, Anxiety and Depression Scale (HADS). BMC Psychiatry 12:6
Fries JF, Spitz P, Kraines RG et al (1980) Measurement of patient outcomes in arthritis. Arthritis Rheum 23:137–145
Beck AT, Ward CH, Mendelson M et al (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:53–63
n a (2002)Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation and treatment of high blood cholesterol in adults (Adult treatment panel III). Final report. Circulation 106:3143–3421
Wilson PW, D’Agostino RB, Levy D et al (1998) Prediction of coronary heart disease using risk factor categories. Circulation 97(18):1837–1847
Cunha VR de, Brenol CV, Brenol JC et al (2012) Metabolic syndrome prevalence is increased in rheumatoid arthritis patients and is associated with disease activity. Scand J Rheumatol 41(3):186–191
Chung CP, Oeser A, Solus JF et al (2008) Prevalence of the metabolic syndrome is increased in rheumatoid arthritis and is associated with coronary atherosclerosis. Atherosclerosis 196(2):756–763
Andersson CX, Gustafson B, Hammarstedt A et al (2008) Inflamed adipose tissue, insulin resistance and vascular injury. Diabetes Metab Res Rev 24:595–603
Panoulas VF, Metsios G, Pace AV et al (2008) Hypertension in rheumatoid arthritis. Rheumatology 47:1286–1298
Kontny E, Plebanczyk M, Lisowska B et al (2012) Comparison of rheumatoid articular adipose and synovial tissue reactivity to proinflammatory stimuli: contribution to adipocytokine network. Ann Rheum Dis 71:262–267
Ehling A, Schaffler A, Herfarth H et al (2006) The potential of adiponectin in driving arthritis. J Immunol 176:4468–4478
Hotamisligil GS, Shargill NS, Spiegelman BM (1993) Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science 259(5091):87–91
Kershaw EE, Flier JS (2004) Adipose tissue as an endocrine organ. J Clin Endocrinol Metab 89(6):2548–2556
Halberg N, Wernstedt-Asterholm I, Scherer PE (2008) The adipocyte as an endocrine cell. Endocrinol Metab Clin North Am 37(3):753–768
Kitahara K, Kusunoki N, Kakiuchi T et al (2009) Adiponectin stimulates IL-8 production by rheumatoid synovial fibroblasts. Biochem Biophys Res Commun 378:218–223
Stofkova A (2009) Leptin and adiponectin: from energy and metabolic dysbalance to inflammation and autoimmunity. Endocr Regul 43:157–168
Luk T, Malam Z, Marshall JC (2008) Pre-B cell colony-enhancing factor (PBEF)/visfatin: a novel mediator of innate immunity. J Leukoc Biol 83:804–816
Rabe K, Lehrke M, Parhofer KG et al (2008) Adipokines and insulin resistance. Mol Med 14(11–12):741–751
Yamauchi T, Nio Y, Maki T et al (2007) Targeted disruption of AdipoR1 and AdipoR2 causes abrogation of adiponectin binding and metabolic actions. Nat Med 13(3):332–339
Niswender KD, Magnuson MA (2007) Obesity and the beta cell: lessons from leptin. J Clin Invest 117:2753–2756
Amaro IF, Gonzalez FD, Junanatey CG et al (2011) Insulin resistance and rheumatoid arthritis. Rheumatol Clin 7(2):124–129
Kim HJ, Higashimori T, Park SY et al (2004) Differential effects of interleukin-6 and -10 on skeletal muscle and liver insulin action in vivo. Diabetes 53:1060–1067
Van der Poll T, Romijn JA, Endert E et al (1991) Tumor necrosis factor mimics the metabolic response to acute infection in healthy humans. Am J Physiol 261:457–465
Pagano G, Bruno A, Cavallo-Perin P et al (1989) Glucose intolerance after short-term administration of corticosteroids in healthy subjects. Prednisone, deflazacort, and betamethasone. Arch Intern Med 149:1098–1101
Dessein PH, Tobias M, Veller MG (2006) Metabolic syndrome and subclinical atherosclerosis in rheumatoid arthritis. J Rheumatol 33:2425–2432
Swinkels D, Demacker P, Hendriks J et al (1989) Low density lipoprotein subfractions and relationship to other risk factors for coronary artery disease in healthy individuals. Arteriosclerosis 9:604–613
Robertson J, Peters MJ, McInnes IB et al (2013) Changes in lipid levels with inflammation and therapy in RA: a maturing paradigm. Nat Rev Rheumatol 9:513–23
Gonzalez-Gay MJ, Gonzlaez-Juanatey C (2014) Inflammation and lipid profile in rheumatoid arthritis: bridging an apparent paradox. Ann Rheum Dis 73:1281–1283
Georgiadis AN, Papavasiliou EC, Lourida ES et al (2006) Atherogenic lipid profile is a feature characteristic of patients with early rheumatoid arthritis: effect of early treatment, a prospective, controlled study. Arthritis Res Ther 8:R82
Corti MC, Salive ME, Guralnik JM (1996) Serum albumin and physical function as predictors of coronary heart disease mortality and incidence in older persons. J Clin Epidemiol 49(5):519–526
Frank RG, Beck NC, Parker JC et al (1988) Depression in rheumatoid arthritis. J Rheumatolol 15:920–925
Hawley DJ, Wolfe F (1988) Anxiety and depression in patients with rheumatoid arthritis: a prospective study of 400 patients. J Rheumatol 15(6):932–941
Katz PP, Yelin EH (1995) The development of depressive symptoms among women with rheumatoid arthritis. Arthritis Rheum 38:49–56
Luppino FS, Wit LM de, Bouvy PF et al (2010) Overweight, obesity and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry 67(3):220–229
Nichols M, Townsend N, Scarborough P et al (2014) Cardiovascular disease in Europe 2014: epidemiological update. Eur Heart J 35:2950–2959
Compliance with ethical guidelines
Conflict of interest. P. Ostojic and D. Bartolovic state that there are no conflicts of interest.
All studies on humans described in the present manuscript were carried out with the approval of the responsible ethics committee and in accordance with national law and the Helsinki Declaration of 1975 (in its current, revised form). Informed consent was obtained from all patients included in studies.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ostojic, P., Bartolovic, D. Disease activity, obesity, functional disability, and depression in patients with rheumatoid arthritis. Z Rheumatol 75, 716–722 (2016). https://doi.org/10.1007/s00393-015-1661-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00393-015-1661-7