
Abstract
Background
Maximal hyperemia is a critical prerequisite for correct fractional flow reserve (FFR) measurements. Continuous administration of adenosine by femoral venous access is considered the gold-standard. However, antecubital venous access is used as an alternative route of administration due to the increasing popularity of radial versus femoral access for coronary catheterization. Because of a potentially larger cross sectional venous area in the arm—theoretically associated with slower flow velocities—and the extremely short half-life of adenosine, there are concerns whether this route of administration is truly equivalent to the femoral route.
Methods
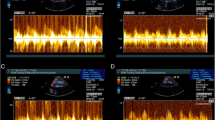
Fifty randomly selected patients with coronary artery disease were included. FFR was measured with a pressure monitoring wire and the recording was digitally stored. Hyperemia was successively induced by adenosine via the antecubital vein at a dose of 140 μg kg−1 min−1 (A140), via the antecubital vein at a dose of 170 μg kg−1 min−1 (A170), and via the femoral vein at a dose of 140 μg kg−1 min−1 (F140).
Results
Induction of hyperemia by A140 yielded significantly lower hyperemic responses than compared with A170 (P = 0.038) and F140 (P = 0.005). No significant difference was seen between adenosine administration by A170 versus F140. Hyperemic stimulation by A140 underestimated lesion severity near the ischemic threshold of FFR more frequently than the other modalities. There were no differences in side-effects between any of the dosages and routes of administration.
Conclusions
The intravenous application of adenosine via antecubital venous access is feasible but slightly less effective than the femoral approach. In this setting, an antecubital dosage of 170 μg kg−1 min−1 is comparable to the standard dosage of 140 μg kg−1 min−1 in the femoral vein. In some patients, this regimen might prevent an underestimation of lesion severity.

Similar content being viewed by others


References
Wilson RF, Wyche K, Christensen BV et al (1990) Effects of adenosine on human coronary arterial circulation. Circulation 82:1595–1606
Van Der Voort PH, van Hagen E, Hendrix G et al (1996) Comparison of intravenous adenosine to intracoronary papaverine for calculation of pressure-derived fractional flow reserve. Cathet Cardiovasc Diagn 39:120–125
Kern MJ, Deligonul U, Tatineni S et al (1991) Intravenous adenosine: continuous infusion and low dose bolus administration for determination of coronary vasodilator reserve in patients with and without coronary artery disease. J Am Coll Cardiol 18:718–729
Pijls NH, De Bruyne B, Peels K et al (1996) Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med 334:1703–1708
Casella G, Leibig M, Schiele TM et al (2004) Are high doses of intracoronary adenosine an alternative to standard intravenous adenosine for the assessment of fractional flow reserve? Am Heart J 148:590–595
Kern MJ, Lerman A, Bech JW et al (2006) Physiological assessment of coronary artery disease in the cardiac catheterization laboratory: a scientific statement from the American Heart Association Committee on Diagnostic and Interventional Cardiac Catheterization, Council on Clinical Cardiology. Circulation 114:1321–1341
Jeremias A, Filardo SD, Whitbourn RJ et al (2000) Effects of intravenous and intracoronary adenosine 5′-triphosphate as compared with adenosine on coronary flow and pressure dynamics. Circulation 101:318–323
Zijlstra F, Juilliere Y, Serruys PW et al (1988) Value and limitations of intracoronary adenosine for the assessment of coronary flow reserve. Cathet Cardiovasc Diagn 15:76–80
De Bruyne B, Pijls NH, Barbato E et al (2003) Intracoronary and intravenous adenosine 5′-triphosphate, adenosine, papaverine, and contrast medium to assess fractional flow reserve in humans. Circulation 107:1877–1883
World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects (2000) JAMA 284:3043–3045
Pijls NH, van Schaardenburgh P, Manoharan G et al (2007) Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J Am Coll Cardiol 49:2105–2111
Legalery P, Schiele F, Seronde MF et al (2005) One-year outcome of patients submitted to routine fractional flow reserve assessment to determine the need for angioplasty. Eur Heart J 26:2623–2629
Fearon WF, Tonino PA, De Bruyne B et al (2007) Rationale and design of the fractional flow reserve versus angiography for multivessel evaluation (FAME) study. Am Heart J 154:632–636
Silber S, Albertsson P, Aviles FF et al (2005) Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology. Eur Heart J 26:804–847
Doesch C, Seeger A, Hoevelborn T et al (2008) Adenosine stress cardiac magnetic resonance imaging for the assessment of ischemic heart disease. Clin Res Cardiol 97:905–912
Pijls NH, Kern MJ, Yock PG et al (2000) Practice and potential pitfalls of coronary pressure measurement. Catheter Cardiovasc Interv 49:1–16
Downey HF, Bashour FA, Boatwright RB et al (1975) Uniformity of transmural perfusion in anesthetized dogs with maximally dilated coronary circulations. Circ Res 37:111–117
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lindstaedt, M., Bojara, W., Holland-Letz, T. et al. Adenosine-induced maximal coronary hyperemia for myocardial fractional flow reserve measurements: comparison of administration by femoral venous versus antecubital venous access. Clin Res Cardiol 98, 717–723 (2009). https://doi.org/10.1007/s00392-009-0056-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-009-0056-7