
Summary
Background and objectives
Management of acute ST-elevation myocardial infarction (STEMI) demands rapid and complete reflow to the infarct related artery (IRA). Primary PCI (percutaneous coronary intervention) performed by experienced operators is superior to thrombolytic thrombolytic therapy and reduces mortality, occurrence of non-fatal reinfarction and stroke, but is not available in rural Germany. We established a regional infarction-network using established therapeutic guidelines comprising of 1 interventional center and 7 referring community hospitals without PCI facilities.
Patients and methods
We analyzed 322 patients with STEMI treated by PCI within the network; 160 patients were transferred from a community hospital without PCI facilities (transfer group (TG): 63.4 yrs., 71.8% men) and 162 patients were admitted directly to the interventional center (center group (CG): 61.7 yrs., 73.8% men). The interval from onset of symptoms to first medical contact was 205 minutes in TG, and 195 minutes in CG (n.s.); 7.8% of the CG and 7.2% of the TG patients were in cardiogenic shock; 95% of patients completed 12- months of follow-up.
Results
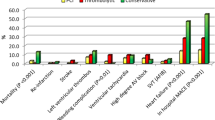
In the TG, median transportation time to PCI was 54 minutes. PCI of the infarct-related artery (IRA) was performed in 95.1% of TG patients and in 94.1% of CG patients. In addition, 96% of all patients received a GP IIb/IIIa receptor inhibitor. In case of pre-interventional application of GP IIb/IIIa receptor inhibitor 22.3% of patients revealed TIMI-3 flow of the IRA before PCI. After PCI, normalized flow to the IRAwas documented in 87.5% of CG versus 86.3% of TG. There were no differences between groups with respect to infarct size (TG vs. CG: CK 2482 vs. 2481 U/I; CKMB 302 vs. 264 U/I), mortality (30 days: 5.3 vs. 5.2%, 6 months: 7.3 vs. 7.1%, 12 months: 7.9 vs. 7.8%); NYHA (1.41 vs. 1.43) and left ventricular ejection fraction (0.41 vs. 0.43).
Conclusions
The organization of a regional STEMI-network with logistic alliance of community hospitals and one experienced interventional center ensures timely PCI treatment of patients with STEMI according to present guidelines even in rural areas, and relegates thrombolytic treatment to bail-out scenarios only.
Zusammenfassung
Hintergrund und Fragestellung
Die Therapie des akuten ST-Hebungsinfarkts (STEMI) verlangt eine unverzügliche und effiziente Reperfusion der infarktrelevanten Koronararterie (IRA). Die primäre PCI („percutaneous coronary intervention“) ist der Lysetherapie bezüglich Mortalität, Häufigkeit von Reinfarkten und Schlaganfallrisiko überlegen, jedoch in Deutschland nicht flächendeckend verfügbar. Nach der Gründung eines regionalen Infarktnetzwerks mit standardisierten Therapierichtlinien zwischen einem PCI-Zentrum und 7 Kliniken der Primärversorgung werden aktuell Verlauf und Prognose der im Netzwerk behandelten Patienten mit STEMI vorgestellt.
Patienten und Methode
Wir analysierten 322 Patienten mit Akut-PCI bei STEMI; 160 Patienten nach Transfer aus einem Zentrum der Primärversorgung (Transfergruppe=TG: 63,4 Jahre, 71,8% Männer) werden mit 162 Patienten mit direkter Aufnahme im PCI-Zentrum (Zentrumsgruppe=ZG: 61,7 Jahre, 73,8% Männer) verglichen. Das Zeitintervall zwischen Symptombeginn und Arztkontakt betrug in der TG 205, in der ZG 195 min; 7,8% der ZG- und 7,2% TG-Patienten befanden sich im kardiogenen Schock. Eine komplette Nachbeobachtung über 12 Monate liegt für 95% der Patienten vor.
Ergebnisse
Die Transportzeit der TG zur Akut-PCI betrug durchschnittlich 54 min. Bei 95,1% der Patienten der TG und 94,4% der ZG erfolgte eine Akut-PCI. 96% aller PCI-Patienten erhielten additiv einen GPIIb/IIIa-Antagonisten. Bereits vor PCI zeigten 22,3% der Patienten mit präinterventioneller Gabe des GPIIb/IIIa-Antagonisten einen TIMI-3-Fluss in der IRA auf. Nach PCI erreichten 87,5% der ZG- und 86,3% der TG-Patienten einen TIMI-3 Fluss. Beide Gruppen zeigten im Verlauf keinen Unterschied hinsichtlich Myokardnekrose (TG vs. ZG: CK 2482 vs. 2481 U/l, CKMB 302 vs. 264 U/l), Mortalität (30 Tage: 5,3 vs. 5,2%, 6 Monate: 7,3 vs. 7,1%, 12 Monate 7,9 vs. 7,8%), NYHA-Stadium (1,41 vs. 1,43) und linksventrikulärer Ejektionsfraktion nach 6 Monaten (0,41 vs. 0,43).
Fazit
Der Aufbau eines regionalen Infarktnetzwerks mit Verknüpfung von Krankenhäusern der Primärversorgung mit einem erfahrenen PCI-Zentrum gestattet unter Verzicht auf eine Lysetherapie eine leitliniengerechte und optimierte Therapie von Patienten mit STEMI. Im Netzwerk erfahren die Patienten der Krankenhäuser ohne Herzkatheterlabor einen adäquaten Behandlungsstandard und Prognose wie Patienten mit primärer Aufnahme im PCI-Zentrum.
Similar content being viewed by others


References
Andersen HR, Nielsen TT, Rasmussen K et al. for the DANAMI-2 Investigators (2003) The Danish Multicenter Randomized Trial on Thrombolytic Therapy versus Acute Coronary Angioplasty in Acute Myocardial Infarction. New Engl J Med 8:349–356
Antoniucci D, Migliorini A, Parodi G et al (2004) Abciximab-supported infarct artery stent implantation for acute myocardial infarction and long-term survival: a prospective, multicenter, randomized trial comparing infarct artery stenting plus abciximab with stenting alone. Circulation 109(14):1704–1706
Bonnefoy E, Lapostolle F, Leizorovicz A et al (2002) Primary angioplasty versus prehospital fibrinolysis in acute myocardial infarction: a randomised study. Comparison of Angioplasty and Prehospital Thrombolysis in Acute Myocardial Infarction (CAPTIM) study group. Lancet 360:825–829
Bonnefoy E, Steg PG, Cabaud S et al. (2005) Is primary angioplasty more effective than prehospital fibrinolysis in diabetics with acute myocardial infarction? Data from the CAPTIM randomised clinical trial. Eur Heart J 26 (17):1712–1718
Hamm CW, Arntz HR, Bode C et al (2004) Leitlinien Akutes Koronarsyndrom Teil 2: Akutes Koronarsyndrom mit ST-Hebung. Z Kardiol 93:324–341
Keeley EC, Boura JA, Grines CL (2003) Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomized trials. Lancet 361:13–20
Montalescot G, Barragan P, Wittenberg O et al for the ADMIRAL investigators (2002) Platelet glycoprotein IIb/IIIa inhibition with coronary stenting for acute myocardial infarction. N Engl J Med 344:1895–1903
Ross AM, Coyne KS, Reiner JS et al (1999) A randomized trial comparing primary angioplasty with a strategy of short-acting thrombolysis and immediate planned rescue angioplasty in acute myocardial infarction: the PACT trial. PACT investigators. Plasminogen-activator Angioplasty Compatibility Trial. J Am Coll Cardiol 34:1954–1962
Schömig A, Kastrati A, Dirschinger J et al (2000) Coronary stenting plus platelet glycoprotein IIb/IIIa blockade compared with tissue plasminogen activator in acute myocardial infarction. Stent versus Thrombolysis for Occluded Coronary Arteries in Patients with Acute Myocardial Infarction Study Investigators. N Engl J Med; 343:385–391
Steg PG, Bonnefoy E, Chaubaud S et al (2003) Impact of time to treatment on mortality after prehospital fibrinolysis or primary angioplasty. Circulation 108:2851–2856
Verheugt FW (2001) GP IIB/IIIA blockers with and without thrombolytic agent in prehospital treatment of acute myocardial infarction. Thromb Res Sep 30;103 [Suppl 1]:113–116. Review
Vermeer F, Ophuis AJ, Berg EJ et al (1999) Prospective randomised comparison between thrombolysis, rescue PCI, and primary PCI in patients with extensive myocardial infarction admitted to a hospital without PCI facilities: a safety and feasibility study. Heart 82:426-431
Widimsky P, Budesinsky T, Vorac D et al (2003) ‘PRAGUE’ Study Group Investigators Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial-PRAGUE-2. Eur Heart J 24:94–104
Widimsky P, Groch L, Zelizko M et al (2000) Multicentre randomized trial comparing transport to primary angioplasty vs immediate thrombolysis vs combined strategy for patients with acute myocardial infarction presenting to a community hospital without a catheterization laboratory. The PRAGUE study. Eur Heart J 21:823–831
Zahn R, Schiele R, Schneider S et al (2002) Clinical practice of primary angioplasty for the treatment of acute myocardial infarction in Germany: results from the MITRA and MIR registries. Z Kardiol 91 [Suppl 3]:64–71
Author information
Authors and Affiliations
Consortia
Additional information
* Drip & Ship-Netzwerk: Universität Rostock, Abteilung Kardiologie der Klinik und Poliklinik für Innere Medizin; Südstadtklinikum Rostock; KMG Klinik Güstrow; Boddenkliniken Ribnitz-Damgarten; Warnow-Klinik Bützow; DRK-Krankenhaus Teterow; Krankenhaus Bad Doberan; Städtisches Krankenhaus Wismar
Rights and permissions
About this article
Cite this article
Schneider, H., Weber, F., Paranskaja, L. et al. Interventionelle Therapie und 1-Jahres Follow up des akuten ST-Hebungsinfarkts im Netzwerk. ZS Kardiologie 94 (Suppl 4), iv85–iv89 (2005). https://doi.org/10.1007/s00392-005-1418-4
Issue Date:
DOI: https://doi.org/10.1007/s00392-005-1418-4