
Abstract
Background
The implementation of a computerized physician order entry (CPOE) can help reduce prescription errors in clinical practice.
Objective
The aim of this study was to evaluate the effects of a CPOE for geriatric patients with the two most common conditions for drug-induced iatrogenic diseases, dysphagia and renal failure.
Subjects and methods
A retrospective analysis of actual drug prescriptions versus CPOE recommendations in the geriatric department of the St. Marien Hospital in Cologne, Germany was carried out. Actual drug prescriptions were collected for 26 patients with dysphagia (15 female, 11 male, average age 82.3 ± 8.0 years) and 35 patients with renal failure (23 female, 12 male, average age 80.5 ± 6.7 years) which were compared with recommended prescriptions by means of a CPOE and discrepancies were statistically analyzed.
Results
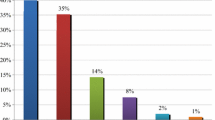
Prescription errors for at least 1 drug were detected in 46 % of patients with renal failure and the administration of at least 1 drug with inadequate crushing was observed in 77 % of dysphagia patients.
Conclusion
Prescription errors appear to be frequent to highly frequent in the medical routine even in a highly specialized geriatric setting. Inaccuracies might be reduced by the implementation of a CPOE and even more if coupled to a decision support system. Drug-drug or drug-disease interactions, which are particularly high risks in patients with multimorbidities, multidrug therapy, renal failure or malnutrition, might be kept under control through careful verification of medication indications, organ function status as well as drug administration and preparation in cases of tube feeding.
Zusammenfassung
Hintergrund
Die Implementierung eines elektronischen Verordnungssystems („computerized physician order entry, CPOE“) kann Ärzte dabei unterstützen Verschreibungsfehler in der klinischen Praxis zu vermeiden.
Ziel
Ziel der Studie war die Evaluation der Effekte eines CPOE für geriatrische Patienten mit den 2 häufigsten Störungen, bei denen es zu medikamentös induzierten iatrogenen Erkrankungen kommen kann: Dysphagie und Niereninsuffizienz.
Material und Methoden
Die Studie fand auf einer akutgeriatrischen Station des St. Marien-Hospitals in Köln statt. Um die Fehlerhäufigkeit beim Verordnen von Arzneistoffen, deren Dosierung bei Niereninsuffizienz anzupassen ist, und bei hinsichtlich der Gabe bei Dysphagiepatienten problematischen Medikamenten zu ermitteln, wurden Verschreibungen retrospektiv mit einem CPOE überprüft. Dafür wurden die erfolgten Verordnungen für 26 Patienten mit Dysphagie (15 w, 11 m, 82,3 ± 8,0 Jahre) und 35 Patienten mit Niereninsuffizienz (23 w, 12 m, 80,5 ± 6,7 Jahre) verglichen mit den Empfehlungen des Programms, die Diskrepanzen wurden statistisch analysiert.
Ergebnisse
Mindestens einen Verordnungsfehler gab es bei 46 % der Niereninsuffizienzpatienten. Die Gabe mindestens eines Medikamentes, das unzureichend zerkleinert worden war, wurde bei 77 % der Dysphagiepatienten beobachtet.
Schlussfolgerung
Die Rate an Verordnungsfehlern scheint bei den untersuchten Patientenpopulationen recht hoch zu sein, obwohl die Analyse in einer auf Geriatrie spezialisierten Fachklinik stattfand. Die Implementierung eines CPOE, vor allem in Kombination mit einem Entscheidungsunterstützungssystem, könnte den Prozess der Verschreibung robuster gegenüber Fehlern machen. Pharmakologische Interaktionen und Kontraindikationen, für die bei geriatrischen Patienten aufgrund Multimorbidität bzw. Multimedikation und bei Patienten mit Niereninsuffizienz oder Mangelernährung ein besonders hohes Risiko besteht, können kontrolliert werden durch sorgfältige Verifizierung der Indikation, des funktionellen Organstatus sowie der Anwendung und der Vorbereitung des Medikaments für per Sonde ernährte Patienten.
Similar content being viewed by others


References
Amann U, Schmedt N, Garbe E (2012) Prescribing of potentially inappropriate medications for the elderly: an analysis based on the PRISCUS list. Dtsch Arztebl Int 109(5):69–75
Aras S, Varli M, Uzun B, Atli T, Keven K, Turgay M (2012) Comparison of different glomerular filtration methods in the elderly: which formula provides better estimates? Ren Fail 34(4):435–41
Budnitz DS, Lovegrove MC, Shehab N, Richards CL (2011) Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med 365:2002–2012
Cockroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16:31–41
Daniels SK, Brailey K, Priestly DH, Herrington LR, Weisberg LA, Foundas AL (1998) Aspiration in patients with acute stroke. Arch Phys Med Rehabil 79(1):14–19
DosingGmbH (2014) AiDKlinik®. http://www.aidklinik.de/. Accessed 15 March 2015
Gallagher P, O`Mahony D (2008) STOPP (Screening Tool of Older Persons’potentially inappropriate Prescriptions): application to acutely ill elderly patients and comparison with Beers’ criteria. Age Ageing 37:673–679
Holt S, Schmiedl S, Thürmann PA (2010) Potentially inappropriate medications in the elderly: the PRISCUS List. Dtsch Arztebl Int 107(31–32):543–551
Kelly J, Wright D, Wood J (2011) Medicine administration errors in patients with dysphagia in secondary care: a multi-centre observational study. J Adv Nurs 67 (12):2615–2627
Long CL, Raebel MA, Price DW, Magid DJ (2004) Compliance with dosing guidelines in patients with chronic kidney disease. Ann Pharmacother 38:853–858
Papaioannou A, Clarke JA, Campbell G, Bedard M (2000) Assessment of adherence to renal dosing guidelines in long-term care facilities. J Am Geriatr Soc 48:1470–1473
Permpongkosol S (2011) Iatrogenic disease in the elderly: risk factors, consequences, and prevention. Clin Interv Aging 6:77–82
Pfaff A (2015) Pharmatrix. http://www.pharmatrix.de/cms/front_content.php?idcat=12. Accessed 15 March 2015
Pirmohamed M, James S, Meakin S, Green C, Scott AK, Walley TJ, Farrar K, Park BK, Breckenridge AM (2004) Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18820 patients. BMJ 329:15–19
Pretorius RW, Gataric G, Swedlund SK, Miller JR (2013) Reducing the risk of adverse drug events in older adults. Am Fam Physician 87(5):331–336
Roberts GW, Ibsen PM, Schiøler CT (2009) Modified diet in renal disease method overestimates renal function in selected elderly patients. Age Ageing 38:698–703
Rochon PA, Field TS, Bates DW, Lee M, Gavendo L, Erramuspe-Mainard J, Judge J, Gurwitz JH (2005) Computerized physician order entry with clinical decision support in the long-term care setting: insights from the Baycrest Centre for Geriatric Care. J Am Geriatr Soc 53:1780–1789
Salomon L, Deray G, Jaudon MC, Chebassier C, Bossi P, Launay-Vacher V, Diquet B, Ceza JM, Levu S, Bruecker G, Ravaud P (2003) Medication misuse in hospitalized patients with renal impairment. Int J Qual Health Care 15(4):331–335
Simon SR, Keohane CA, Amato M, Coffey M, Cadet B, Zimlichman E, Bates DW (2013) Lessons learned from implementation of computerized provider order entry in 5 community hospitals: a qualitative study. BMC Med Inform DecisMak 13:67
SPSS Inc (2008) SPSS Statistics for Windows, Version 17.0. Chicago
Stuerzlinger H, Hiebinger C, Pertl D, Traurig P (2009) Computerized physician order entry—effectiveness and efficiency of electronic medication ordering with decision support systems. GMS Health Technol Assess 86(1):2
Syed S, Wang D, Goulard D, Rich T, Innes G, Lang E (2013) Computer order entry systems in the emergency department significantly reduce the time to medication delivery for high acuity patients. Int J Emerg Med 6(1):20
Terrell KM, Perkins AJ, Hui SL, Callahan CM, Dexter PR, Miller DK (2010) Computerized decision support for medication dosing in renal insufficiency: a randomized, controlled trial. Ann Emerg Med 56:623–629
Tosato M, Landi F, Martone AM, Cherubini A, Corsonello A, Volpato S, Bernabei R, Onder G (2014) Potentially inappropriate drug use among hospitalised older adults: results from the CRIME study. Age Ageing 43(6):767–773
Vendome Health Care Media (2015) Healthcare informatics. http://www.healthcare-informatics.com. Accessed 15 March 2015
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S. Frisse, G. Röhrig, J. Franklin, M.C. Polidori and R-J. Schulz declare that there are no conflicts of interest.
All studies on humans described in the present manuscript were carried out with the approval of the ethics committee of the University of Cologne and in accordance with national law and the Helsinki Declaration of 1975 (in its current, revised form).
Additional information
M.C. Polidori und R-J. Schulz were equal supervisors.
Rights and permissions
About this article

Cite this article
Frisse, S., Röhrig, G., Franklin, J. et al. Prescription errors in geriatric patients can be avoided by means of a computerized physician order entry (CPOE). Z Gerontol Geriat 49, 227–231 (2016). https://doi.org/10.1007/s00391-015-0911-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00391-015-0911-2