
Summary
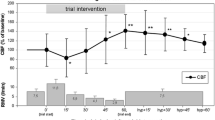
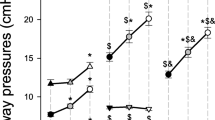
Objective The aim of our study was to investigate the effects of these new strategies [the new approach by Amato et al. (NAA) and the modified “open lung” concept (OLC)] on cerebral perfusion using an animal model. Method After inducing ARDS with a thorax contusion, 38 pigs (German Edelschwein), divided into two groups, were mechanically ventilated either with NAA or OLC over a 24 h period. Measurements of intracranial pressure (ICP), cerebral perfusion pressure (CPP), intracerebral partial pressure of oxygen (ptiO2) and transcranial Doppler ultrasound (TCD) were conducted. Results In the NAA group with a tolerance of paCO2 up to 80 mm Hg (permissive hypercapnia) a fast increase of ICP by 11.5█5.4mm Hg (p<0.05) and a consecutive moderate decrease of CPP were observed. The elevated ICP was detected throughout the study period. The ptiO2 increased significantly from 49█39mm Hg to 84█24mm Hg. The TCD showed an increase of systolic, diastolic and mean flow velocities. In the OLC group a brief increase of ICP and a decrease of CPP were observed during the initial recruitment maneuvre (<60 s). The TCD showed a decrease in flow velocities followed by a rapid increase. The ICP rose from 14.0█5.4 mm Hg to 19█6.2 mm Hg (p<0.05) and returned to baseline values after one hour. There was no evidence of critical increase of ICP during the study period. The ptiO2 rose significantly. No negative effects of high-PEEP level were observed. Conclusion Patients with ARDS or acute lung injury additionally suffering from cerebrovascular diseases should be treated by a respiratory strategy without permissive hypercapnia, because of the negative effects of permissive hypercapnia on ICP in the NAA group. The hyperventilation that ensues with the “open lung” concept attenuates the permissive hypercapnia. There was no increase in ICP and no longer significant decrease in CPP using the “open lung” concept. There was no evidence of negative effects of PEEP levels of up to 16–20 cm H2O.
Zusammenfassung
Ziel unserer Studie waren Untersuchungen zu Auswirkungen aktueller Respiratorstrategien (New Approach n. Amato-(NAA), modifiziertes „Open lung-Konzept” n. Lachmann-(OLC) auf die zerebrale Perfusion nach experimentellem Thoraxtrauma im Tiermodell. Material und Methode Bei 38 Versuchstieren (Deutsches Edelschwein), eingeteilt in 2 Gruppen (NAA-und OLC-Gruppe) erfolgte über einen 24-stündigen Untersuchungszeitraum (nach Thoraxtrauma) eine intraparenchymatöse Hirndruck (ICP)-und Sauerstoffpartialdruckmessung (ptiO2) sowie eine dopplersonographische Exploration der A. carotis interna sinistra (ICA li.). Neben einer invasiven kontinuierlichen RR-und Pulmonalisdruckmessung erfolgte eine online-Blutgasanalyse (Paratrend®). Ergebnisse Im Rahmen des NAA (permissive Hyperkapnie bis 80 mmHg) sind ICP-Steigerung um bis zu 11,5█5,4mmHg (p<0,05) zu konstatieren. Der ptiO2 stieg von 49█39mmHg auf 84█24mmHg. Der dopplersonographische Verlauf zeigte am extrakraniellen Gefäßsystem (ICA) eine Zunahme der Flusswerte. Beim modifiziertem OLC sind diese Veränderung nicht zu konstatieren. Im Verlauf einer kurzzeitigen Erhöhung des PIP (ca. 65mbar) kommt es dopplersonograpisch zum Abfall der Flusswerte (diastolischem Nullfluss) für die Zeit des OLM (<60 s). Der mittlere arterielle Blutdruck (MAP) fiel von 84█15mmHg kurzzeitig auf Werte von 58█11,4 mmHg (p<0,05). Der ICP erhöhte sich unter dem OLC von 14,0█5,4 mmHg auf 19█6,2 mmHg (n.s.). Krisenhafte ICP-Steigerungen waren in einem 24-stündigem Beobachtungsintervall nicht nachzuweisen. Eine Hyperkapnie trat nicht auf. Der intraparenchymatös gemessene ptiO2 steigerte im Verlauf der Untersuchung signifikant. Es waren keine negativen Auswirkungen hoher PEEP-Level zu konstatieren. Schlussfolgerungen Beatmungsstrategien mit Aktzeptanz permissiver Hyperkapnie und konsekutiver Erhöhung des ICP scheinen für Patienten mit gestörter zerebrovaskulärer Autoregulation problematisch. Durch ein Respiratorregime, welches eine Hyperkapnie sicher verhindert, lässt sich eine negative Beeinflussung der zerebralen Perfusion vermeiden. Durch eine balancierte respiratorische Alkalose (bei angestrebten Ziel-paCO2-Werten zwischen 28–35 mmHg) gelingt es einen Hirndruckanstieg zu verhindern.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Author information
Authors and Affiliations
Additional information
Eingegangen: 26. Januar 2001 Akzeptiert: 12. März 2001
Rights and permissions
About this article
Cite this article
Mende, L., Katscher, S., Engelmann, L. et al. Hämodynamische Auswirkungen aktueller Beatmungsverfahren auf die zerebrale Perfusion. Intensivmed 38, 394–401 (2001). https://doi.org/10.1007/s003900170060
Issue Date:
DOI: https://doi.org/10.1007/s003900170060