
Abstract
Objectives
Cardiogenic shock (CS) remains the leading cause of death in patients hospitalized for acute myocardial infarction (AMI). Historically, conventional therapy has been associated with a 90% mortality rate. Several studies have demonstrated the importance of early revascularization strategies for lowering mortality. The additional use of intra-aortic balloon counterpulsation (IABP) provides incremental benefit to reperfusion therapy. Therefore, this study reviews our experience of infarct-related CS treatment with early aggressive combined use of revascularization and IABP.
Methods
Retrospectively, 50 consecutive patients (36 male) with CS complicating AMI, admitted to our department during 2005 and 2006, were analyzed. Mean age was 68.9 years. All patients underwent early coronary angiography with an option of percutaneous coronary intervention (PCI), and IABP was implanted immediately after the procedure.
Results
In-hospital mortality, as the primary outcome measure of the study, was 42%. CS presented with ST elevation MI (STEMI) in 50%, as non-STEMI (NSTEMI) in 50%. Upon admission, 30% of CS had required cardiopulmonary resuscitation (CPR), 72% were on mechanical ventilation, and 10% acquired prehospital thrombolysis. Single coronary vessel disease (CVD) presented in 18%, dual CVD in 18%, and triple CVD in 64% of CS. Average left ventricular ejection fraction (EF) was 27.9%. There were no significant differences concerning the EF in the CS subgroups STEMI vs. NSTEMI and non-survivors vs. survivors. PCI was successfully performed in 88% of CS, one patient underwent IABP and then was submitted to emergency CABG. Clinically significant signs of sepsis were present in 32%, the more in the non-survivor group (48% vs. 21%, p < 0.05).
Conclusion
Our data suggest that a treatment strategy with early aggressive combined use of revascularization and IABP can also improve survival in high-risk patients with CS complicating AMI.
Zusammenfassung
Hintergrund
Der kardiogene Schock (KS) stellt die Haupttodesursache bei akutem Myokardinfarkt (AMI) dar. Mit rein konservativer Therapie liegt die Mortalität bei 90%. Durch frühzeitige Revaskularisierungsmaßnahmen wie Koronarintervention (PCI) und Bypass-OP konnte die Letalität auf 50–70% gesenkt werden. Der prognostische Wert zusätzlicher kreislaufunterstützender Maßnahmen mittels intraaortaler Ballon-Gegenpulsations-Pumpe (IABP) ist bisher nicht eindeutig geklärt. Die aktuellen internationalen Leitlinien sprechen derzeit eine Empfehlung für den Einsatz der IABP erst bei fehlender Stabilisierung der Kreislaufsituation durch Pharmaka aus. Die vorliegende Studie fasst die eigenen Erfahrungen eines alternativen Therapiekonzepts mit frühzeitig kombiniertem Einsatz von PCI und IABP in Hinblick auf die intrahospitale Mortalität zusammen und versucht prognostisch ungünstige Prädiktoren zu identifizieren.
Methoden
Retrospektiv wurden 50 Patienten (P.) (36 Männer) mit KS analysiert, die in den Jahren 2005 und 2006 aufgrund eines AMI in unsere Klinik aufgenommen wurden. Das mittlere Alter lag bei 68,9 Jahren. Die Patienten wurden frühestmöglich der Koronarangiographie mit PCI-Option zugeführt und unmittelbar postinterventionell noch im Herzkatheterlabor mit einer IABP versorgt.
Ergebnisse
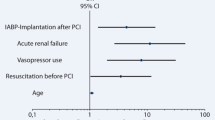
Die intrahospitale Mortalität als primärer Endpunkt der Studie betrug 42%. 25 P. (50%) wiesen einen STEMI, 25 P. (50%) einen NSTEMI auf. 15 P. (30%) wurden präklinisch, 8 P. (16%) periinterventionell reanimiert. 5 P. (10%) wurden präklinisch lysiert, 36 P. (72%) waren invasiv beatmet. Bei 9 P. (18%) zeigte sich eine Eingefäß-KHK, bei 9 (18%) eine Zweigefäß-KHK und bei 32 (64%) eine Dreigefäß-KHK. Die mittlere linksventrikuläre Ejektionsfraktion (EF) bei Aufnahme lag bei 27,9%. Es fanden sich keine signifikanten Unterschiede der EF bei P. mit STEMI vs. NSTEMI und Tod vs. Überleben. Eine PCI erfolgte bei 44 P. (88%), 1 P. erhielt die IABP zur Überbrückung bis zur Bypass-OP. Zeichen einer SIRS/Sepsis wiesen 16 P. (32%) auf, dabei signifikant häufiger in der Gruppe der verstorbenen Patienten (48% vs. 21%, p < 0,05). Weitere Prädiktoren für ein schlechtes Outcome waren NSTEMI, invasive Beatmung, periinterventionelle Reanimation und akutes Nierenversagen mit Dialysepflichtigkeit.
Schlussfolgerungen
Bei Patienten mit infarktbedingtem KS führte eine aggressive, frühzeitig kombinierte Therapie, bestehend aus Revaskularisation und Implantation der IABP, zu einer Absenkung der Intrahospital- Mortalität unter 50%. Als prognostisch ungünstige Faktoren wurden eine systemische Inflammation sowie die Faktoren NSTEMI, periinterventionelle Reanimation, invasive Beatmung und akutes Nierenversagen mit Dialysepflichtigkeit identifiziert.
Similar content being viewed by others


Abbreviations
- AMI:
-
Akuter Myokardinfarkt
- CPR:
-
Kardiopulmonale Reanimation
- CVVH:
-
Chronisch veno-venöse Hämofiltration
- Gef.:
-
Gefäß
- HD:
-
Hämodialyse
- IABP:
-
Intraaortale Ballon-Gegenpulsationspumpe
- KH:
-
Krankenhaus
- KHK:
-
Koronare Herzerkrankung
- KS:
-
Kardiogener Schock
- LVEF:
-
Linksventrikuläre Ejektionsfraktion
- MODS:
-
Multiorgandysfunktion
- MOV:
-
Multiorganversagen
- NA:
-
Notarzt
- NSTEMI:
-
Nicht-ST-Strecken-Hebungsinfarkt
- PCI:
-
Perkutane Koronarintervention
- präkl.:
-
präklinisch
- SIRS:
-
Systemic inflammatory response syndrome
- STEMI:
-
ST-Strecken-Hebungsinfarkt
Literatur
Antman EM, Anbe AT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC, Alpert JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK, Ornato JP (2004) ACC/ AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation 110:588–636
Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS (2005) Trends in management and outcome of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA 294:448–454
Chen EW, Canto JG, Parsons LS, Petersen ED, Littrell KA, Every NR, Gibson CM, Hochman JS, Ohman M, Cheeks M, Barron HV (2003) Relation between hospital intra-aortic balloon counterpulsation volume and mortality in acute myocardial infarction complicated by cardiogenic shock. Circulation 108:951–957
The CREATE-ECLA Trial Group (2005) Effect of glucose-insulin-potassium infusion on mortality in patients with acute ST-segment elevation myocardial infarction: the CREATE-ECLA randomized controlled trial. JAMA 293:437–446
Dauerman HL, Goldberg RJ, White K, Gore JM, Sadiq I, Gurfinkel E, Budaj A, de Sa EL, Lopez-Sendon J, for the CRACE Investigators (2002) Revascularization, stenting, and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. Am J Cardiol 90:838–842
Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeLemtel TH (1999) Early revascularization in acute myocardial infarction complicated by cardiogenic shock. N Engl J Med 341:625–634
Hochman JS (2003) Cardiogenic shock complicating acute myocardial infarction: expanding the paradigm. Circulation 107:2998–3002
Hochman JS, Sleeper LA, Webb JG, Dzavik V, Buller CE, Aylward P, Col J, White HD, for the SHOCK Investigators (2006) Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA 295:2511–2515
Jacobs AK, French JK, Col J, Sleeper LA, Slater JN, Carnendran L, Boland J, Jiang X, LeLemtel T, Hochman JS (2000) Cardiogenic shock with non- ST-segment elevation myocardial infarction: a report from the SHOCK trial registry. J Am Coll Cardiol 36:1091–1096
Jeger RV, Tseng CH, Hochman JS, Bates ER (2006) Interhospital transfer for early revascularization in patients with ST-elevation myocardial infarction complicated by cardiogenic shock – a report from the SHOCK trial and registry. Am Heart J 152:686–692
Jeger RV, Harkness SM, Ramanathan K, Buller CE, Pfisterer ME, Sleeper LA, Hochman JS (2006) Emergency revascularization in patients with cardiogenic shock on admission: a report from the SHOCK trial and registry. Eur Heart J 27:664–670
Kohsaka S, Menon V, Lowe AM, Lange M, Dzavik V, Sleeper LA, Hochman JS (2005) Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock. Arch Intern Med 165:1643–1650
Kohsaka S, Menon V, Iwata K, Lowe A, Sleeper LA, Hochman JS (2007) Microbiological profile of septic complication in patients with cardiogenic shock following acute myocardial infarction (from the SHOCK study). Am J Cardiol 99:802–804
Mann HJ, Nolan PE (2006) Update on the management of cardiogenic shock. Curr Opin Crit Care 12:431–436
Nieminen MS, Böhm M, Cowie MR, Drexler H, Fillipatos GS, Gendeau G, Hasin Y, Lopez-Sendon J, Mebazaa A, Metra M, Rhodes A, Swedberk K (2005) Executive summary of the guidelines on the diagnosis and treatment of acute heart failure. Eur Heart J 26:384–416
Trost JC, Hillis LD (2006) Intra-aortic balloon counterpulsation. Am J Cardiol 97:1391–1398
Webb JG, Sleeper LA, Buller CE, Boland J, Palazzo A, Buller E, White HD, Hochman JS (2000) Implications of the timing of cardiogenic shock after acute myocardial infarction: a report from the SHOCK trial registry. J Am Coll Cardiol 36:1084–1090
Weiss AT, Engel S, Gotsman CJ, Shefer A, Hasin Y, Bitran D, Gotsman MS (1984) Regional and global left ventricular function during intra-aortic balloon counterpulsation in patients with acute myocardial infarction shock. Am Heart J 108:249–254
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Andrié, R.P., Lickfett, L., Skowasch, D. et al. Frühzeitiger kombinierter Einsatz von Revaskularisation und intraaortaler Ballon-Gegenpulsation bei kardiogenem Schock im Rahmen eines akuten Myokardinfarkts. Intensivmed 45, 463–470 (2008). https://doi.org/10.1007/s00390-008-0874-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00390-008-0874-2