
Abstract
Background and aims
This study compared outcome following the two common surgical procedures for anorectal melanoma: wide local excision and abdominal perineal resection. We also examined the utility of endoluminal ultrasound to guide therapy.
Patients and methods
Records of 19 patients surgically treated at our institution were studied. In addition to type of surgical procedure, we noted age, metastatic disease spread, sphincter involvement, tumor size and thickness, and mode of diagnosis. Survival after diagnosis and after recurrence of disease were also recorded. Ultrasound was used in seven, with the lesion delineated in six (all had therapy guided by the ultrasound). Regarding surgery ten had wide local excision, seven had abdominal perineal resection, and two had other procedures.
Results
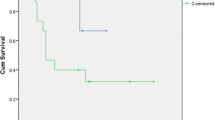
The most common sites of recurrence were distant in 31.6% and regional lymph nodes in 26.3%. Mean survival after recurrence was 13 months (range 5–29). Two patients who had wide local excision are disease free and alive 135 and 29 months after diagnosis. Neither surgical treatment conferred obvious benefit on survival.
Conclusion
Ultrasound can guide management by delineating lesions amendable to wide local excision. Since the mortality rate is high, wide local excision offers the advantage of avoiding a permanent colostomy and should be considered the procedure of choice when excision is feasible.
Similar content being viewed by others

References
Moore WD (1857) Recurrent melananosis of the rectum after previous removal from the verge of the anus in a man aged 65. Lancet I:290–294
Wanebo HJ, Woodruff JM, Farr CH, Quan SH (1981) Anorectal melanoma. Cancer 47:1891–1900
Slingluff CL Jr, Vollmer RT, Seigler HF (1990) Anorectal melanoma: clinical characteristics and results of surgical management in 24 patients. Surgery 107:1–9
Thibault C, Sagar P, Nivatvongs S, lstrup DM, Wolff BG (1997) Anorectal melanoma—an incurable disease? Dis Colon Rectum 40:661–668
Pack GT, Oropeza R (1967) A comparative study of melanoma and epidermoid carcinoma of the anal canal: a review of 20 melanomas, and 29 epidermoid carcinomas (1930 to 1965). Dis Colon Rectum 10:161–176
Brady MS, Kavolius JP, Quan SH (1995) Anorectal melanoma: a 64-year experience at Memorial Sloan-Kettering Cancer Center. Dis Colon Rectum 38:146–151
Ross M, Pezzi C, Pezzi T, Meurer D, Hickey R, Balch C (1990) Patterns of failure in anorectal melanoma. A guide to surgical therapy. Arch Surg 125:313–316
Ward MWN, Romano G, Nicholls RJ (1986) The surgical treatment of anorectal malignant melanoma. Br J Surg 73:68–69
Lange J (2001) Melanoma. In: Cameron JL (ed) Current surgical therapy. Mosby, St Louis, pp 1208–1212
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Malik, A., Hull, T.L. & Floruta, C. What is the best surgical treatment for anorectal melanoma?. Int J Colorectal Dis 19, 121–123 (2004). https://doi.org/10.1007/s00384-003-0526-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-003-0526-8