
Abstract
Purpose
To identify risk factors that can predict prevalence of anastomotic strictures (AS) following esophageal atresia (EA) repair.
Methods
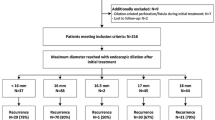
Of 46 consecutive patients with EA managed at our institution between 2004 and 2012, 35 underwent esophageal anastomosis and were included in this retrospective longitudinal study. Routine endoscopy was performed 1 month after surgical repair. According to stricture index (SI), endoscopically calculated as SI = (D − d)/D, where D is the diameter of the esophageal pouch and d the stricture diameter, population was divided into Group 1, SI ≤ 0.1 (no evidence of stricture); Group 2, 0.3 > SI > 0.1 (mild stricture); Group 3, SI ≥ 0.3 (high-grade stricture). Trends of subsequent endoscopic esophageal dilatations were compared between the groups using Wilcoxon–Mann–Whitney or Pearson’s tests. Cox regression analysis was performed to estimate the hazard ratio.
Results
Gastro-esophageal reflux disease (P = 0.04), tension on the anastomosis (P = 0.02) and long-gap form (P = 0.008) have an increased risk of developing AS. SI at 1 month after surgery correlates with the average number of future dilatations: Group 2 and 3 compared to Group 1 required more dilatations (hazard ratio 2.291 and 12.765).
Conclusion
AS remain frequent complications of esophageal surgery, especially in specific subgroups of patients. SI at 1 month after surgery could already predict the severity of the stricture and the need for subsequent endoscopic esophageal dilatations.
Similar content being viewed by others


Abbreviations
- AS:
-
Anastomotic strictures
- EA:
-
Esophageal atresia
- HR:
-
Hazard ratio
- SD:
-
Standard deviation
- SI:
-
Stricture index
References
Goyal A, Jones MO, Couriel JM et al (2006) Esophageal atresia and trachea-esophageal fistula. Arch Dis Child Fetal Neonatal Ed 91(5):F381–F384
Deurloo JA, Ekkelkamp S, Schorl M et al (2002) Esophageal atresia: historical evolution and result in 371 patients. Ann Thorac Surg 73(1):267–272
Chittmittrapap S, Spitz L, Kiely EM et al (1992) Anastomotic leakage following surgery for esophageal atresia. J Pediatr Surg 27(1):29–32
Serhal L, Gottrand F, Sfeir R et al (2012) Anastomotic stricture after surgical repair of esophageal atresia: frequency, risk factors, and efficacy of esophageal bougie dilatations. J Pediatr Surg 45(7):1459–1462
Spitz L (1996) Esophageal atresia: past, present and future. J Pediatr Surg 31(1):19–25
Spitz L (2006) Esophageal atresia. lesson I have learned in a 40-year experience. J Pediatr Surg 41(10):1635–1640
Said M, Mekki M, Golli M et al (2003) Balloon dilatation of anastomotic strictures secondary to surgical repair of esophageal atresia. Br J Radiol 76(901):26–31
Spitz L (2007) Esophageal atresia. Orphanet J Rare Dis 11:2–24
Harmon CM, Coran AG (2006) Congenital Anomalies of the Esophagus. In: Grosfeld JL (ed) Pediatric Surgery, 6th edn. Philadelphia, Pennsylvania, pp 1051–1078
Spitz L, Hitchcock RJ (1994) Oesophageal atresia and tracheo-oesophageal fistula. In: Freeman NV, Burge DN, Griffiths M, Malone PSJ (eds): Surgery of the Newborn. Churchill Livingstone, pp 353–373
Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, Sondheimer J, Staiano A, Thomson M, Veereman-Wauters G, Wenzl TG, North American Society for Pediatric Gastroenterology Hepatology and Nutrition, European Society for Pediatric Gastroenterology Hepatology and Nutrition (2009) Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr 49(4):498-547
Zhao R, Li K, Shen C, Zheng S (2011) The outcome of conservative treatment for anastomotic leakage after surgical repair of esophageal atresia. J Pediatr Surg 46(12):2274–2278
Kim IO, Yeon KM, Kim WS et al (1993) Perforation complicating balloon dilatation of esophageal strictures in infants and children. Radiology 189(3):741–744
Koivusalo A, Pakarinen MP, Rintala JP (2004) Is routine dilatation after repair of esophageal atresia with distal fistula better than dilatation when symptoms arise? comparison of results of two European pediatric surgical center. J Pediatr Surg 39:1643–1647
Pregun I, Hritz I, Tulassay Z et al (2009) Peptic esophageal stricture: medical treatment. Dig Dis 27(1):31–37
Ferguson DD (2005) Evaluation and management of benign esophageal strictures. Dis Esophagus 18(6):359–364
Lee M, Kubik CM, Polhamus CD et al (1995) Preliminary experience with endoscopic intralesional steroid injection therapy for refractory upper gastrointestinal strictures. Gastrointest Endosc 41(6):598–601
Ramage JI Jr, Rumalla A, Baron TH et al (2005) A prospective, randomized, double-blind, placebo-controlled trial of endoscopic steroid injection therapy for recalcitrant esophageal peptic strictures. Am J Gastroenterol 100(11):2419–2425
Acknowledgments
No funding was necessary for this study.
Conflict of interest
The authors have no conflict of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Parolini, F., Leva, E., Morandi, A. et al. Anastomotic strictures and endoscopic dilatations following esophageal atresia repair. Pediatr Surg Int 29, 601–605 (2013). https://doi.org/10.1007/s00383-013-3298-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-013-3298-4