
Abstract
Purpose
This study compared laparoscopy-assisted stoma closure (Lap) with conventional closure (Co) to assess loss of intestine.
Methods
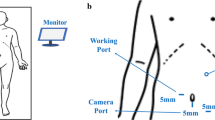
Ileostomies (loop L; single S) were performed 5 cm proximal to the ileocecal junction through a right lower quadrant incision in forty 11-week-old Lewis rats (L = 20, S = 20). Stoma closure was performed 60 days later using laparoscopy (Lap) or conventional closure (Co) in 10 rats each, to give 4 groups, Lap-L, Lap-S, Co-L, and Co-S. End-to-end anastomosis was performed through the stoma site in all rats. Bowel resected from the skin to the anastomosis was termed resected unusable bowel (RUB) and measured blindly. Laparotomy was performed 30 days later to assess the status of the anastomosis and complications.
Results
Average RUB with Lap was significantly shorter; Lap-L (17.8 mm) versus Co-L (23.8 mm), P = 0.002, and Lap-S (10.6 mm) versus Co-S (13.8 mm), P = 0.001. During Co, accidental full-thickness injury to underlying bowel during stoma take-down occurred in 3 Co-L and 2 Co-S rats. All Lap rats were uncomplicated. Average times taken until end of stoma take-down were 6.1 min for Lap-L (3.2 min for trocar insertion, 2.8 min for stoma take-down), 5.6 min for Lap-S (2.8 and 2.7 min), 6.3 min for Co-L (from first incision to stoma take-down), and 5.1 min for Co-S (P = NS). At laparotomy there was no evidence of complications such as wound infection, incisional hernia or anastomotic stenosis in any rat.
Conclusions
Our results suggest that laparoscopy-assisted stoma closure is safe and quick, and results in less loss of intestine during stoma closure.
Similar content being viewed by others


References
Miyano G, Yanai T, Okazaki T et al (2007) Laparoscopy-assisted stoma closure. J Laparoendosc Adv Surg Tech A 17:395–398
Miyano G, Okawada M, Yanai T et al (2009) Outcome of stoma closure in children: a comparison of laparoscopy-assisted and conventional open techniques. J Laparoendosc Adv Surg Tech A
Anadol AZ, Topgul K (2006) Santulli enterostomy revisited: indications in adults. World J Surg 30:1935–1938
Sapin E, Carricaburu E, De Boissieu D et al (1999) Conservative intestinal surgery to avoid short-bowel syndrome in multiple intestinal atresias and necrotizing enterocolitis: 6 cases treated by multiple anastomoses and Santulli-type enterostomy. Eur J Pediatr Surg 9:24–28
Garcia-Botello SA, Garcia-Armengol J, Garcia-Granero E et al (2004) A prospective audit of the complications of loop ileostomy construction and takedown. Dig Surg 21:440–446
Wong KS, Remzi FH, Gorgun E et al (2005) Loop ileostomy closure after restorative proctocolectomy: outcome in 1, 504 patients. Dis Colon Rectum 48:243–250
Turan C, Ozdemir M (2004) The effect of intestinal plication on intestinal transit time in rats. Pediatr Surg Int 20:425–428
Vanamo K, Rintala R, Lindahl H (2004) The Santulli enterostomy in necrotising enterocolitis. Pediatr Surg Int 20:692–694
Singh M, Owen A, Gull S et al (2006) Surgery for intestinal perforation in preterm neonates: anastomosis vs stoma. J Pediatr Surg 41:725–729
Berry DP, Scholefield JH (1997) Closure of loop ileostomy. Br J Surg 84:524
Feldman JD, Woda BA (1980) Pathology and tumor incidence in aged Lewis and BN rats. Clin Immunol Immunopathol 15:331–343
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Miyano, G., Ichikawa, S., Lane, G.J. et al. Loss of intestine during stoma closure: an experimental model comparing laparoscopic and conventional techniques. Pediatr Surg Int 26, 119–121 (2010). https://doi.org/10.1007/s00383-009-2513-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-009-2513-9