
Abstract
Background and Aim
Botox injection treatment (BIT) is a potentially effective but yet unproven treatment of functional anal outlet obstruction that is caused by non-relaxing internal anal sphincter. We present a single institution experience of BIT from 2005 to 2008.
Patients and methods
Sixteen patients (11 males), eight with Hirschsprung’s disease (HD) (one with total colon aganglionosis, TCA) and eight with internal sphincter achalasia (ISA) were included. Median ages were 3.8 years (0.4–9.3) for HD and 8.1 years (range 1.5–11.4) for ISA. ISA was defined as the absence of rectoanal inhibitory reflex with normal rectal biopsies. Seven HD patients had previous coloanal pull-through (CAPT), and one (TCA) colectomy and ileoanal J-Pouch anastomosis. Two of the ISA patients had undergone internal sphincter myectomy and two had Malone procedure [antegrade colonic enema (ACE)]. Indication for BIT in 16 patients was anal outlet obstruction (n = 11) with soiling and recurring HD-associated enterocolitis (n = 5) and in one patient (HD, TCA) soiling with enterocolitis (n = 1). Before BIT, all patients underwent anorectal manometry, rectal biopsies and barium enema. The effect of BIT was evaluated after 2 months and BIT was repeated if necessary. Effect of BIT was scored as follows: 0 no, 1 little, 2 significant effect and 3 symptoms disappeared.
Results
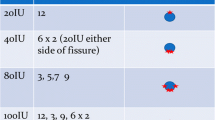
Median follow-up was 19 months (range 3–43). The median number of injections was two per patient (range 1–4) and the median Botox dose was 80 U (range 40–100). Scores of BIT effect were 3 or 2 in five (31%) and 0 or 1 in 11 (69%). After adjunctive treatment modalities (myectomy n = 1, CAPT n = 1, adjusted ACE/laxative treatment), the end result was good or satisfactory in 11 (69%) but remained poor in 5 (31%) patients. Patient age, diagnosis, anorectal resting pressure or findings in barium enema were not correlated with BIT efficiency score (R range −0.06 to 0.39, P = 0.12–0.91).
Conclusion
Although successful in some patients, the role of BIT remains undetermined. It is difficult to predict which patients will profit from BIT. Continuing other treatment modalities after BIT may improve the results.
Similar content being viewed by others

References
Langer JC (2004) Persistent obstructive symptoms after surgery for Hirschsprung’s disease: development of a diagnostic and therapeutic algorithm. J Pediatr Surg 39:1458–1462
Ciamarra P, Nurko S, Barksdale E, Fishman S, Di Lorenzo C (2003) Internal anal sphincter achalasia in children: clinical characteristics and treatment with Clostridium botulinum toxin. J Pediatr Gastroenterol Nutr 37:315–319
Zaslavsky C, Loening-Baucke V (2003) Anorectal manometric evaluation of children and adolescents postsurgery for Hirschsprung’s disease. J Pediatr Surg 38:191–195
Wildhaber BE, Pakarinen M, Rintala RJ, Coran AG, Teitelbaum DH (2004) Posterior myotomy/myectomy for persistent stooling problems in Hirschsprung’s disease. J Pediatr Surg 39:920–926
Heikkinen M, Lindahl H, Rintala RJ (2005) Long-term outcome after internal sphincter myectomy for internal sphincter achalasia. Pediatr Surg Int 21:84–87
Messineo A, Codrich D, Monai M, Martellossi S, Ventura A (2001) The treatment of internal anal sphincter achalasia with botulinum toxin. Pediatr Surg Int 17:521–523
Irani K, Rodriguez L, Doody DP, Goldstein AM (2008) Botulinum toxin for the treatment of chronic constipation in children with internal anal sphincter dysfunction. Pediatr Surg Int 24:779–783
Chumpitazi BP, Fishman SJ, Nurko S (2009) Long-term clinical outcome after botulinum toxin injection in children with nonrelaxing internal anal sphincter. Am J Gastroenterol 104:976–983
Hosseini SM, Foroutan HR, Bahador A, Khosravi MB, Geramizadeh B, Sabet B, Zeraatian S, Razmi T, Banani SJ (2008) Role of rectal biopsy in predicting response to intrasphincteric botulinum toxin injection for obstructive symptoms after a pullthrough operation. Indian J Gastroenterol 27:99–102
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koivusalo, A.I., Pakarinen, M.P. & Rintala, R.J. Botox injection treatment for anal outlet obstruction in patients with internal anal sphincter achalasia and Hirschsprung’s disease. Pediatr Surg Int 25, 873–876 (2009). https://doi.org/10.1007/s00383-009-2438-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-009-2438-3