
Abstract
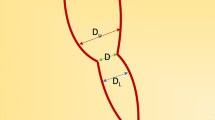
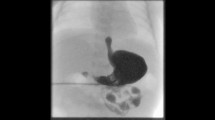
Anastomotic tension with the potential to lead to post-operative complication is usually evaluated using gap length before anastomosis in patients with esophageal atresia and a distal tracheoesophageal fistula (EA with a TEF). However a uniform, accurate measurement of gap length is not possible and estimation of the length the delicate distal esophageal stump is stretched by the anastomosis may have greater utility. The aim of this paper was to propose a novel method to evaluate the anastomotic tension in EA with a TEF. Forty consecutive patients having EA with a TEF were studied. Primary anastomosis without gastrostomy was performed in all cases. When the TEF was cut off, the most proximal site of the tracheal side was marked using a tiny metallic clip. When anastomosis was completed, the distance from the clip to the anastomotic site was measured as the stretched length. On the esophagram taken subsequently, the same distance was measured, together with the distance from the clip to the esophago-cardiac junction as the original distal esophageal length. The stretching ratio was calculated by dividing the former by the latter. The stretched length on esophagram (median: 3.0 mm, range: −12 to 21) was significantly correlated with that measured during surgery (median: 2.3 mm, range; −14 to 15) (r=0.96, P<0.0001). The median of original distal esophageal lengths was 60.0 mm (range: 35–80). The stretching ratio was significantly correlated with the stretched length, and the number of the stretching ratio as a percentage corresponded to about double the number of the stretched length on esophagram in millimeters (y=1.91x+0.58, r=0.98, P<0.0001). Anastomotic leakage and recurrence of TEF were not experienced. In patients complicated with gastroesophageal reflux (GER), the site of TEF was significantly more distal as compared with the other cases [median (range): 5.0th (4.0–6.0) vs 3.5th (1.5–5.0) thoracic vertebral level, P<0.009]. The stretched length and the stretching ratio were also longer and larger, respectively [median (range): 10.0 mm (6–21) vs 2.0 (−12 to 14) mm, P<0.008, 17.3% (12.7–47.7) vs 2.9% (−16.4 to 29.8)%, P<0.018). Similar tendencies were observed for patients complicated with stricture. Estimation of the stretched length of the distal esophageal stump is useful to evaluate the anastomotic tension. If the stretched length is more than 10 mm, it will be necessary to consider the possibility that stricture or GER may arise afterwards.




Similar content being viewed by others

References
Healey PJ, Sawin RS, Hall DG et al (1998) Delayed primary repair of esophageal atresia with tracheoesophageal fistula: is it worth the wait? Arch Surg 133:552–556
Foker JE, Linden BC, Boyle EM Jr et al (1997) Development of a true primary repair for the full spectrum of esophageal atresia. Ann Surg 226:533–541
Brown AK, Tam PK (1996) Measurement of gap length in esophageal atresia: a simple predictor of outcome. J Am Coll Surg 182:41–45
Sillen U, Hagberg S, Rubenson A et al (1988) Management of esophageal atresia: review of 16 years’ experience. J Pediatr Surg 23:805–809
Santos AD, Thompson TR, Johnson DE et al (1983) Correction of esophageal atresia with distal tracheoesophageal fistula. J Thorac Cardiovasc Surg 85:229–236
Lessin MS, Wesselhoeft CW, Luks FI et al (1999) Primary repair of long-gap esophageal atresia by mobilization of the distal esophagus. Eur J Pediatr Surg 9:369–372
Davison P, Poenaru D, Kamal I (1999) Esophageal atresia: primary repair of a rare long gap variant involving distal pouch mobilization. J Pediatr Surg 34:1881–1883
Boyle EM Jr, Irwin ED, Foker JE (1994) Primary repair of ultra-long-gap esophageal atresia: results without a lengthening procedure. Ann Thorac Surg 57:576–579
Hands LJ, Dudley NE (1986) A comparison between gap-length and Waterston classification as guides to mortality and morbidity after surgery for esophageal atresia. J Pediatr Surg 21:404–406
Tanaka S, Nagaya M, Kato J et al (1997) Efficacy of elective ventilator care for post-operative management of TEF. J Jpn Assoc Pediatr Surg 33:962–963
Chittmittrapap S, Spitz L, Kiely EM et al (1990) Anastomotic stricture following repair of esophageal atresia. J Pediatr Surg 25:508–511
Bishop PL, Klein MD, Philippart AI et al (1985) Transpleural repair of esophageal atresia without a primary gastrostomy: 240 patients treated between 1951 and 1983. J Pediatr Surg 20:823–828
Ein SH, Shandling B, Wesson D et al (1989) Esophageal atresia with distal tracheoesophageal fistula: associated anomalies and prognosis in the 1980s. J Pediatr Surg 24:1055–1059
Spitz L, Kiely EM, Morecroft JA et al (1994) Oesophageal atresia: at-risk groups for the 1990’s. J Pediatric Surg 29:723–725
Driver CP, Shanker KR, Jones MO et al (2001) Phenotypic presentation and outcome of esophageal atresia in the era of the Spitz classification. J Pediatr Surg 36:1419–1421
Louhimo I, Lindahl H (1983) Esophageal atresia: primary results of 500 consecutively treated patients. J Pediatr Surg 18:217–229
Al-Salem AH, Qaisaruddin S, Srair HA et al (1997) Elective, postoperative ventilation in the management of esophageal atresia and tracheoesophageal fistula. Pediatr Surg Int 12:261–263
Chittmittrapap S, Spitz L, Brereton RJ et al (1993) Postoperative elective ventilation in babies with “marked anastomotic tension” after repair of esophageal atresia. J Med Assoc Thai 76:683–687
McKinnon LJ, Kosloske AM (1990) Prediction and prevention of anastomotic complications of esophageal atresia and tracheoesophageal fistula. J Pediatr Surg 25:778–781
Filston HC, Rankin JS, Grimm JK (1984) Esophageal atresia. Prognostic factors and contribution of preoperative telescopic endoscopy. Ann Surg 199:532–537
Myers NA, Beasley SW, Auldist AW (1990) Secondary esophageal surgery following repair of esophageal atresia with distel tracheoesohageal fistula. J Pediatr Surg 25:773–777
Montedonico S, Diez-Pardo JA, Possogel AK et al (1999) Effects of esophageal shortening on the gastroesophageal barrier: an experimental study on the causes of reflux in esophageal atresia. J Pediatr Surg 34:300–303
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nagaya, M., Kato, J., Niimi, N. et al. Proposal of a novel method to evaluate anastomotic tension in esophageal atresia with a distal tracheoesophageal fistula. Ped Surgery Int 21, 780–785 (2005). https://doi.org/10.1007/s00383-005-1540-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-005-1540-4