
Abstract
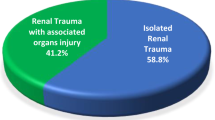
A retrospective analysis of the medical records of 205 children with renal injuries secondary to blunt abdominal trauma is used to make recommendations regarding the initial diagnostic and therapeutic approaches in this type of patient. It was found that the absence of hematuria on initial urinalysis does not exclude a serious renal injury. Thus, following blunt abdominal trauma, all children should undergo imaging procedures to exclude renal injury, whether they have hematuria or not. Ultrasound is a good initial screening procedure in all patients. Computed tomography is recommended for the definitive evaluation of suspected major renal injuries. Since even major renal injuries may heal without surgical intervention, conservative management is the recommended initial treatment of choice. Surgery is reserved for those children who are hemodynamically unstable and those that develop complications.
Similar content being viewed by others

References
Akgur FM, Aktug T, Olguner M, Kovanlikaya A, Hakguder G (1997) Prospective study investigating routine usage of ultrasonography as the initial diagnostic modality for the evaluation of children sustaining blunt abdominal trauma. J Trauma 42:626–628
Bass DH, Semple PL, Cywes S (1991) Investigation and management of blunt renal injuries in children: a review of 11 years’ experience. J Pediatr Surg 26:196–200
Brown SL, Elder JS, Spirnak JP (1998) Are pediatric patients more susceptible to major renal injury from blunt trauma? A comparative study. J Urol 160:138–140
Brown SL, Haas C, Dinchman KH, Elder JS, Spirnak JP (2001) Radiologic evaluation of pediatric blunt renal trauma in patients with microscopic hematuria. World J Surg 25:1557–1560
Carroll PR, McAninch JW (1989) Staging of renal trauma. Urol Clin North Am 16:193–201
Ciftci AO, Tanyel FC, Salman AB, Buyukpamukcu N, Hicsonmez A (1998) Gastrointestinal tract perforation due to blunt abdominal trauma. Pediatr Surg Int 13:259–264
Desai SR, Upadhyay V (2000) Rhabdoid tumour of the kidney: a diagnostic challenge and a fatal outcome. Pediatr Surg Int 16:449–450
Kuzmarov IW, Morehouse DD, Gibson S (1981) Blunt renal trauma in the pediatric population: a retrospective study. J Urol 126:648–649
Livne PM, Gonzales ET Jr (1985) Genitourinary trauma in children. Urol Clin North Am 12:53–65
McAninch JW, Carroll PR, Klosterman PW, Dixon CM, Greenblatt MN (1991) Renal reconstruction after injury. J Urol 145:932–937
Mee SL, McAninch JW, Robinson AL, Auerbach PS, Carroll PR (1989) Radiographic assessment of renal trauma: a 10-year prospective study of patient selection. J Urol 141:1095–1098
Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, Flint LM, Gennarelli TA, Malangoni MA, Ramenofsky ML, Trafton PG (1989) Organ injury scaling: spleen, liver, and kidney. J Trauma 29:1664–1666
Morey AF, Bruce JE, McAninch JW (1996) Efficacy of radiographic imaging in pediatric blunt renal trauma. J Urol 156:2014–2018
Rance CH, Singh SJ, Kimble R (2000) Blunt abdominal trauma in children. J Paediatr Child Health 36:2–6
Russell RS, Gomelsky A, McMahon DR, Andrews D, Nasrallah PF (2001) Management of grade IV renal injury in children. J Urol 166:1049–1050
Smith EM, Elder JS, Spirnak JP (1993) Major blunt renal trauma in the pediatric population: is a nonoperative approach indicated? J Urol 149:546–548
Stein JP, Kaji DM, Eastham J, Freeman JA, Esrig D, Hardy BE (1994) Blunt renal trauma in the pediatric population: indications for radiographic evaluation. Urology 44:406–410
Wessel LM, Scholz S, Jester I, Arnold R, Lorenz C, Hosie S, Wirth H, Waag KL (2000) Management of kidney injuries in children with blunt abdominal trauma. J Pediatr Surg 35:1326–1330
Acknowledgement
We wish to acknowledge Roderick I. Macpherson, Emeritus Professor of Pediatric Radiology, South Carolina, for his critical review of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ceylan, H., Gunsar, C., Etensel, B. et al. Blunt renal injuries in Turkish children: a review of 205 cases. Ped Surgery Int 19, 710–714 (2003). https://doi.org/10.1007/s00383-003-1033-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-003-1033-2