
Abstract
Background
Quadrigeminal cistern arachnoid cysts (QACs) are difficult to treat because of their deep location and the presence of nervous and vascular structures of the pineal–quadrigeminal region. There are several surgical procedures available for QACs, including craniotomy and cyst excision or fenestration, ventriculoperitoneal or cystoperitoneal shunting, and endoscopic fenestration. There is a debate about which method is the best.
Objective
The aim of this study is to evaluate the effectiveness and safety of endoscopic ventriculocystostomy (VC) and third ventriculostomy (ETV) for treatment of arachnoid cysts of the quadrigeminal cistern.
Methods
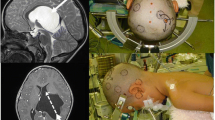
Twenty-eight patients with QACs who had undergone endoscopic treatment in our department between August 2007 and June 2014 were studied retrospectively. Patient age at the time of endoscopic treatment ranged from 5 months to 42 years, including 25 children (14 males and 11 females) and 3 adults (one male and two females). All patients presented with hydrocephalus and did not undergo shunting prior to neuroendoscopic surgery. The first endoscopic procedures included lateral ventricle cystostomy (LVC) together with ETV in 18 cases, third ventricle cystostomy (3rd VC) together with ETV in 3 cases, and double VC (3rd VC and LVC) together with ETV in 7 cases. Data were obtained on clinical and neuroradiological presentation, indications to treat, surgical technique, complications, and the results of clinical and neuroradiological follow-up.
Results
Complete success was achieved in 25 (89.3 %) of 28 cases. During the follow-up period, one case underwent endoscopic reoperation with success. Shunts were implanted in 2 patients due to progression of symptoms and increase in hydrocephalus after the first endoscopic operation. Shunt independency was achieved in 26 (92.9 %) of 28 cases. The cyst was reduced in size in 22 cases (78.6 %). Postoperative images showed a reduction in the size of the ventricles in 23 cases (82.1 %). There was no surgical mortality. Subdural collection developed in 4 cases (14.3 %) and required a transient subduroperitoneal shunt in 2 cases, whereas the other 2 patients were asymptomatic and did not require any surgical treatment.
Conclusions
VC together with ETV through precoronal approach is an effective treatment for symptomatic QACs and should be the initial surgical procedure. The surgical indications should include signs of elevated ICP (including increased head circumference), Parinaud syndrome, gait ataxia, and nystagmus. Also, surgery is indicated by progressive enlargement of the cyst and young children with large cysts even if the patients are asymptomatic. Contraindications to surgery include the absence of symptoms (older children and adult) and isolated developmental delay. The main criterion for successful surgery should be improvement of clinical symptoms instead of reduced cyst volume and/or ventricular size. Repeated endoscopic procedures may be considered only for the patients whose symptoms improved after first endoscopic operation.



Similar content being viewed by others


References
Shim KW, Lee YH, Park EK et al (2009) Treatment option for arachnoid cysts. Childs Nerv Syst 25(11):1459–1466
Greenfield JP, Souweidane MM (2005) Endoscopic management of intracranial cysts. Neurosurg Focus 19(6):E7
Nowosławska E, Polis L, Kaniewska D et al (2006) Neuroendoscopic techniques in the treatment of arachnoid cysts in children and comparison with other operative methods. Childs Nerv Syst 22(6):599–604
Gui SB, Wang XS, Zong XY et al (2011) Assessment of endoscopic treatment for middle cranial fossa arachnoid cysts. Childs Nerv Syst 27(7):1121–1128
Gui SB, Wang XS, Zong XY et al (2011) Suprasellar cysts: clinical presentation, surgical indications, and optimal surgical treatment. BMC Neurol 11:52
Gui S, Zong X, Li C et al (2013) Endoscopic treatment of convexity arachnoid cysts. Childs Nerv Syst 29(3):505–508
Rengachary SS, Watanabe I (1981) Ultrastructure and pathogenesis of intracranial arachnoid cysts. J Neuropathol Exp Neurol 40(1):61–83
Di Rocco C, Caldarelli M (1993) Supratentorial interhemispheric and pineal region cysts. In: Intracranial Cyst Lesions, Raimondi AG, Choux M, Di Rocco C (eds). New York, Berlin: Springer − Verlag Chap 11: 153-168
El-Ghandour NM (2013) Endoscopic treatment of quadrigeminal arachnoid cysts in children. J Neurosurg Pediatr 12(5):521–528
Erşahin Y, Kesikçi H (2009) Endoscopic management of quadrigeminal arachnoid cysts. Childs Nerv Syst 25(5):569–576
Cinalli G, Spennato P, Columbano L et al (2010) Neuroendoscopic treatment of arachnoid cysts of the quadrigeminal cistern: a series of 14 cases. J Neurosurg Pediatr 6(5):489–497
Raffel C, McComb JG (1988) To shunt or to fenestrate: which is the best surgical treatment for arachnoid cysts in pediatric patients? Neurosurgery 23(3):338–342
Ohnishi YI, Fujimoto Y, Taniguchi M et al (2007) Neuroendoscopically assisted cyst-cisternal shunting for a quadrigeminal arachnoid cyst causing typical trigeminal neuralgia. Minim Invasive Neurosurg 50(2):124–127
Gangemi M, Maiuri F, Colella G et al (2005) Endoscopic treatment of quadrigeminal cistern arachnoid cysts. Minim Invasive Neurosurg 48(5):289–292
Garg K, Tandon V, Sharma S et al (2014) Quadrigeminal cistern arachnoid cyst: a series of 18 patients and a review of literature. Br J Neurosurg 12:1–7
Ruge JR, Johnson RF, Bauer J (1996) Burr hole neuroendoscopic fenestration of quadrigeminal cistern arachnoid cyst: technical case report. Neurosurgery 38(4):830–837
Choi JU, Kim DS, Huh R (1999) Endoscopic approach to arachnoid cyst. Childs Nerv Syst 15(6-7):285–291
Sengul G, Tuzun Y, Cakir M et al (2012) Neuroendoscopic approach to quadrigeminal cistern arachnoid cysts. Eurasian J Med 44(1):18–21
Inamasu J, Ohira T, Nakamura Y et al (2003) Endoscopic ventriculo-cystomy for non-communicating hydrocephalus secondary to quadrigeminal cistern arachnoid cyst. Acta Neurol Scand 107(1):67–71
Hayashi N, Endo S, Tsukamoto E et al (1999) Endoscopic ventriculocystocisternostomy of a quadrigeminal cistern arachnoid cyst. Case report. J Neurosurg 90(6):1125–1128
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Rights and permissions
About this article

Cite this article
Gui, S., Bai, J., Wang, X. et al. Assessment of endoscopic treatment for quadrigeminal cistern arachnoid cysts: A 7-year experience with 28 cases. Childs Nerv Syst 32, 647–654 (2016). https://doi.org/10.1007/s00381-015-2962-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-015-2962-5