
Abstract
Introduction
Subdural effusion in an infant is a rare clinical scenario which may be secondary to a variety of etiologies. Massive subdural effusion is an extremely rare complication of head injury.
Case report
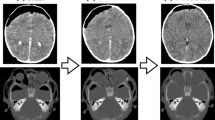
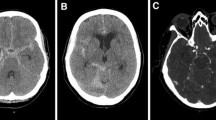
Authors report a rare case of progressive massive subdural effusion which, despite bilateral bur-hole placement and drainage, failed and presented with visual deterioration and massive bulge of the scalp at bur-hole sites, producing a rabbit ear appearance in a 10-month-old infant. Ultimately, cystoperitoneal shunt was carried out in a desperate attempt to prevent impending rupture of scalp sutures at sites of previous bur-hole placement. This was followed by not only complete resolution of hygroma but also visual recovery. The patient is doing well at 6 months following shunt, regaining normal vision and appropriate developmental milestones. A MRI scan of the brain was carried out at last follow-up, which revealed mild ventriculomegaly with the rest of the brain being unremarkable, and subduro-peritoneal shunt in situ. Such a case has not been reported in the literature till date.
Discussion
Subdural effusion usually runs a self-limiting course. Though neurosurgical intervention is occasionally needed, different methods of surgical procedure for management include bur hole alone, bur holes with subdural drain placement, twist drill craniotomy with drain, and even craniotomy. Various methods of management are discussed along with a review of pertinent literature.



Similar content being viewed by others

References
Caldarelli M, Di Rocco C, Romani R (2002) Surgical treatment of chronic subdural hygromas in infants and children. Acta Neurochir (Wien) 144:581–588
Hwang SK, Kim SL (2000) Infantile head injury, with special reference to the development of chronic subdural hematoma. Childs Nerv Syst 16:590–594
Vinchon M, Delestret I, DeFoort-Dhellemmes S, Desurmont M, Noulé N (2010) Subdural hematoma in infants: can it occur spontaneously? Data from a prospective series and critical review of the literature. Childs Nerv Syst 26:1195–1205
Vinchon M, Joriot S, Jissendi-Tchofo P, Dhellemmes P (2006) Postmeningitis subdural fluid collection in infants: changing pattern and indications for surgery. J Neurosurg 104:383–387
Klimo P Jr, Matthews A, Lew SM, Zwienenberg-Lee M, Kaufman BA (2011) Minicraniotomy versus bur holes for evacuation of chronic subdural collections in infants—a preliminary single-institution experience. J Neurosurg Pediatr 8:423–429
Miyake H, Kajimoto Y, Ohta T, Kuroiwa T (2002) Managing subdural fluid collection in infants. Childs Nerv Syst 18:500–504
Abouzari M, Rashidi A, Zandi-Toghani M, Behzadi M, Asadollahi M (2009) Chronic subdural hematoma outcome prediction using logistic regression and an artificial neural network. Neurosurg Rev 32:479–484
Kwon TH, Park YK, Lim DJ, Cho TH, Chung YG, Chung HS et al (2000) Chronic subdural hematoma: evaluation of the clinical significance of postoperative drainage volume. J Neurosurg 93:796–799
Cenic A, Bhandari M, Reddy K (2005) Management of chronic subdural hematoma: a national survey and literature review. Can J Neurol Sci 32:501–506
Lega BC, Danish SF, Malhotra NR, Sonnad SS, Stein SC (2010) Choosing the best operation for chronic subdural hematoma: a decision analysis. J Neurosurg 113:615–621
Mondorf Y, Abu-Owaimer M, Gaab MR, Oertel JMK (2009) Chronic subdural hematoma—craniotomy versus burr hole trepanation. Br J Neurosurg 23:612–616
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Satyarthee, G.D., Dawar, P. & Sharma, B.S. “Rabbit Ear” scalp deformity caused by massive subdural effusion in infant following bilateral bur-hole drainage failure: successfully managed with subduro-peritoneal shunt. Childs Nerv Syst 29, 1993–1996 (2013). https://doi.org/10.1007/s00381-013-2233-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-013-2233-2