
Abstract
Introduction
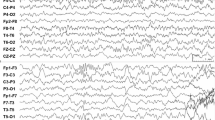
The mechanism of epilepsy in Sturge–Weber syndrome (SWS) has not been elucidated, since it is difficult to detect epileptic discharges on scalp EEG records. To determine the electrophysiological characteristics of SWS, we evaluated epileptic discharges using intracranial electrocorticography (ECoG).
Case summary
We report a 1-year and 3-month-old boy diagnosed with SWS whose psychomotor development was impaired despite good control of his seizures with several antiepileptic drugs (AEDs). Prolonged video ECoG monitoring was performed to determine whether subclinical seizures had induced his developmental delay.
Discussion
Frequent seizures were detected as motionless staring and respiratory distress. His seizures originated from multiple areas along the Sylvian fissure, propagated very slowly, and lasted for 10 to 30 min. Left hemispherotomy was performed, and he was confirmed to be completely seizure-free after surgery. Our findings indicate that long-lasting and barely discernible seizures may continue in patients with SWS who appear to have good control of epilepsy with AEDs.



Similar content being viewed by others


References
Arzimanoglou A, Aicardi J (1992) The epilepsy of Sturge–Weber syndrome: clinical features and treatment in 23 patients. Acta Neurol Scand 140:18–22
Arzimanoglou AA, Andermann F, Aicardi J, Sainte-Rose C, Beaulieu MA, Villemure JG, Olivier A, Rasmussen T (2000) Sturge–Weber syndrome: indications and results of surgery in 20 patients. Neurology 55:1472–1479
Bentson JR, Wilson GH, Newton TH (1971) Cerebral venous drainage pattern of the Sturge–Weber syndrome. Radiology 101:111–118
Bourgeois M, Crimmins DW, de Oliveira RS, Arzimanoglou A, Garnett M, Roujeau T, Di Rocco F, Sainte-Rose C (2007) Surgical treatment of epilepsy in Sturge–Weber syndrome in children. J Neurosurg 106:20–28
Brenner RP, Sharbrough FW (1976) Electroencephalographic evaluation in Sturge–Weber syndrome. Neurology 26:629–632
Coley SC, Britton J, Clarke A (1998) Status epilepticus and venous infarction in Sturge–Weber syndrome. Child’s Nerv Syst 14:693–696
Cure JK, Holden KR, Van Tassel P (1995) Progressive venous occlusion in a neonate with Sturge–Weber syndrome: demonstration with MR venography. AJNR 16:1539–1542
Delalande O, Bulteau C, Dellatolas G, Fohlen M, Jalin C, Buret V, Viguier D, Dorfmuller G, Jambaque I (2007) Vertical parasagittal hemispherotomy: surgical procedures and clinical long-term outcomes in a population of 83 children. Neurosurgery 60:ONS19–ONS32 (discussion ONS32)
Di Rocco C, Tamburrini G (2006) Sturge–Weber syndrome. Child’s Nerv Syst 22:909–921
Jansen FE, van Huffelen AC, Witkamp T, Couperus A, Teunissen N, Wieneke GH, van Nieuwenhuizen O (2002) Diazepam-enhanced beta activity in Sturge–Weber syndrome: its diagnostic significance in comparison with MRI. Clin Neurophysiol 113:1025–1029
Peacock WJ, Wehby-Grant MC, Shields WD, Shewmon DA, Chugani HT, Sankar R, Vinters HV (1996) Hemispherectomy for intractable seizures in children: a report of 58 cases. Child’s Nerv Syst 12:376–384
Probst FP (1980) Vascular morphology and angiographic flow patterns in Sturge–Weber angiomatosis: facts, thoughts and suggestions. Neuroradiology 20:73–78
Sujansky E, Conradi S (1995) Sturge–Weber syndrome: age of onset of seizures and glaucoma and the prognosis for affected children. J Child Neurol 10:49–58
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sugano, H., Nakanishi, H., Nakajima, M. et al. Seizures continue even after prompt anti-epileptic drug medication in Sturge–Weber syndrome—study from prolonged video electrocoticography, a case report. Childs Nerv Syst 25, 143–146 (2009). https://doi.org/10.1007/s00381-008-0696-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-008-0696-3