
Abstract
Introduction
In a small subset of patients, a Chiari malformation can present with signs of raised intracranial pressure due to obstruction of cerebrospinal fluid flow or with the raised intracranial pressure as the primary pathological driving force resulting in tonsillar herniation.
Case report
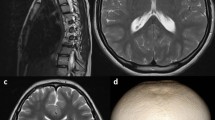
The authors report a unique case in a 14-year-old boy with a Chiari malformation type 1–syringomyelia complex with slit-like ventricles. We have successfully managed the acute presentation of raised intracranial pressure, mimicking idiopathic intracranial hypertension, utilizing a frameless stereotactic image-navigated endoscopic third ventriculostomy alone. We present the preoperative and postoperative radiological and ophthalmological findings and discuss the possible mechanisms related to the pathophysiology and treatment in this case. The patient’s symptoms resolved immediately postoperatively with resolution of papilledema. At 18-month follow-up, the patient remains entirely asymptomatic and the need for craniovertebral decompression appears to have been obviated.
Conclusion
We advocate that in the Chiari malformation type 1–syringomyelia complex with normal or small ventricles, patients presenting with isolated signs and symptoms of raised intracranial pressure alone can be safely and effectively managed with an electromagnetic-guided stereotactic endoscopic third ventriculostomy as a primary treatment option.




Similar content being viewed by others


References
Alberti O, Riegel T, Hellwig D, Bertalanffy H (2001) Frameless navigation and endoscopy. J Neurosurg 95(3):541–543
Alden TD, Ojemann JG, Park TS (2001) Surgical treatment of Chiari I malformation: indications and approaches. Neurosurg Focus 11(1):E2 Review
Azeem SS, Origitano TC (2001) Ventricular catheter placement with a frameless neuronavigational system: a 1-year experience. Neurosurgery 60(4 Suppl 2):243–247 discussion 247–8
Banik R, Lin D, Miller NR (2006) Prevalence of Chiari I malformation and cerebellar ectopia in patients with pseudotumor cerebri. J Neurol Sci 247(1):71–75
Bejjani GK (2003) Association of the adult Chiari malformation and idiopathic intracranial hypertension: more than a coincidence. Med Hypotheses 60(6):859–863
Caldarelli M, Novegno F, Vassimi L, Romani R, Tamburrini G, Di Rocco C (2007) The role of limited posterior fossa craniectomy in the surgical treatment of Chiari malformation type I: experience with a pediatric series. J Neurosurg 106(3 Suppl):187–195
Cinciripini GS, Donahue S, Borchert MS (1999) Idiopathic intracranial hypertension in prepubertal pediatric patients: characteristics, treatment, and outcome. Am J Ophthalmol 127(2):178–182
Erbay SH, O’Callaghan MG, Bhadelia R (2005) Is lumbar puncture contraindicated in patients with Chiari I malformation? AJNR Am J Neuroradiol 26(4):985
Fagan LH, Ferguson S, Yassari R, Frim DM (2006) The Chiari pseudotumor cerebri syndrome: symptom recurrence after decompressive surgery for Chiari malformation type I. Pediatr Neurosurg 42(1):14–19
Gil Z, Siomin V, Beni-Adani L, Sira B, Constantini S (2002) Ventricular catheter placement in children with hydrocephalus and small ventricles: the use of a frameless neuronavigation system. Childs Nerv Syst 18(1–2):26–29
Gumprecht H, Trost HA, Lumenta CB (2000) Neuroendoscopy combined with frameless neuronavigation. Br J Neurosurg 14(2):129–131
Hayhurst C, Osman-Farah J, Das K, Mallucci C (2008) Initial management of hydrocephalus associated with Chiari malformation Type 1–syringomyelia complex via endoscopic third ventriculostomy: an outcome analysis. J Neurosurg 108:1211–1214 (June 2008)
Johnston I, Hawke SH, Halmagyi GM, Teo C (1991) The pseudotumour syndrome: disorders of cerebrospinal fluid circulation causing intracranial hypertension without ventriculomegaly. Arch Neurol 48:740–747
Kamel MH, Mansour N, Kelleher MO, Aquilina K, Young S (2007) Association of intracranial hypertension without ventriculomegaly and Chiari malformation: a dangerous combination. Br J Neurosurg 13:1–3
Kesler A, Fattal-Valevski A (2002) Idiopathic intracranial hypertension in the pediatric population. J Child Neurol 17(10):745–748
Meadows J, Kraut M, Guarnieri M, Haroun RI, Carson BS (2000) Asymptomatic Chiari type I malformations identified on magnetic resonance imaging. J Neurosurg 92:920–926
Milhorat TH, Chou MW, Trinidad EM, Kula RW, Mandell M, Wolpert C, Speer MC (1999) Chiari I malformation redefined: clinical and radiographic findings for 364 symptomatic patients. Neurosurgery 44:1005–1017
Schroeder HW, Wagner W, Tschiltschke W, Gaab MR (2001) Frameless neuronavigation in intracranial endoscopic neurosurgery. J Neurosurg 94(1):72–79
Wellons JC 3rd, Tubbs RS, Bui CJ, Grabb PA, Oakes WJ (2007) Urgent surgical intervention in pediatric patients with Chiari malformation type I. Report of two cases. J Neurosurg 107(1 Suppl):49–52
Woodworth GF, McGirt MJ, Elfert P, Sciubba DM, Rigamonti D (2005) Frameless stereotactic ventricular shunt placement for idiopathic intracranial hypertension. Stereotact Funct Neurosurg 83(1):12–16
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kandasamy, J., Kneen, R., Gladstone, M. et al. Chiari I malformation without hydrocephalus: acute intracranial hypertension managed with endoscopic third ventriculostomy (ETV). Childs Nerv Syst 24, 1493–1497 (2008). https://doi.org/10.1007/s00381-008-0672-y
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-008-0672-y