
Abstract
Introduction
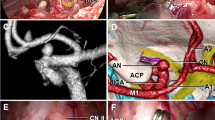
The use of the endoscope (fiberscope) to assist the microsurgical clipping of cerebral aneurysm was first reported by Fischer and Mustafa in 1994. The rigid endoscope has been increasingly used during aneurysm surgery in which structures around the aneurysm can be detected with high quality imaging. Our 3 years of its use now allows us to assess the endoscope’s efficacy and limits in standard surgery with a pterional approach in aneurysms of the anterior circulation. The endoscope can carry out a supportive role in planning surgical manoeuvres and in verifying whether clipping has been performed correctly or not. In our view, among the aneurysms of the anterior circulation, the endoscope is particularly useful in those of the internal carotid and the anterior communicating arteries. In many cases of these aneurysms the posterior communicating artery, choroidal artery or one of the distal cerebral arteries is hidden behind the aneurysm dome. Dome retraction is often required in order to see these vascular structures with the microscope. Thus an endoscope with a 30° view angle becomes very useful. The concealed areas are identified without retraction, which prevents the possibility of the aneurysm being ruptured and also reduces the use of temporary clipping. From its early use as a supportive measure that is sometimes useful in surgery for “easy” aneurysms, the endoscope has now become almost indispensable for the “difficult” aneurysms, including the large and giant ones before and after clipping. Thus, the endoscope should be kept ready for use in the operating theatre for any eventuality.
Objective
We assess the advantages and disadvantages of the use of the endoscope in the microsurgical treatment of intracranial aneurysms.
Methods
During our 3 years of experience, 52 patients with 48 ruptured and 10 unruptured aneurysms of the anterior circulation (including 6 cases of two-fold aneurysms) underwent clipping with endoscope support through a pterional approach. All ruptured aneurysms produced a Hunt and Hess Grade I or II subarachnoid haemorrhage. The endoscope was inserted before and after clipping in order to observe the conditions surrounding the aneurysm and to receive immediate confirmation that clipping had been performed correctly.
Results
In all cases general anatomy visualization was provided by the endoscope, and the correct clip positioning and vessel conditions were easily checked. In 4 cases the endoscope showed that the clip had been positioned incorrectly. Additional clipping was performed in these cases: in 2 cases the clip was re-applied correctly and in another case a clip was added. Only the fourth patient with a large communicating artery died (1.9%) of cerebral infarction. This was due to post-clipping stenosis of one distal cerebral artery in which it was not possible to re-position the clip correctly because of the presence of arteriosclerotic calcific plaque near the aneurysm neck. In 3 cases there was an intraoperative ruptured aneurysm dome that was not caused by the endoscope insertion. No further complications were caused by the endoscope.
Conclusion
In certain cases endoscopic-assisted microsurgery is an exceptional aid to the surgeon and must become part of the operating theatre equipment and kept on hand ready for use. The endoscope is, in our opinion, particularly useful in certain aneurysm localisations (internal carotid artery–anterior communicating artery [ICA–ACOMA]).




Similar content being viewed by others


References
Auer LM, Holzer P, Ascher PW, Heppner F (1988) Endoscopic neurosurgery. Acta Neurochir (Wien) 90:1–14
Chen JC, Moffitt K, Levy ML (1997) Head-mounted display system for microneurosurgery. Stereotact Funct Neurosurg 68:25–32
Fischer J, Mustafa H (1994) Endoscopic-guided clipping of cerebral aneurysms. Br J Neurosurg 8:559–565
Fries G, Perneczky A (1999) Intracranial endoscopy. Adv Tech Stand Neurosurg 25:21–60
Hopf NJ (1999) Endoscopic neurosurgery “around the corner” with a rigid endoscope. Technical note. Minim Invasive Neurosurg 42:27–31
Kakizawa Y, Hongo K, Takasawa H, Miyairi Y, Sato A, Tanaka Y, Kobayashi S (2003) “Real” three-dimensional constructive interference in steady-state imaging to discern microneurosurgical anatomy. Technical note. J Neurosurg 98:625–630
Kalavakonda C, Sekhar LN, Ramachandran P, Hechl P (2002) Endoscope-assisted microsurgery for intracranial aneurysms. Neurosurgery 51:1119–11126; discussion 1126–1127
Kato Y, Sano H, Nagahisa S, Iwata S, Yoshida K, Yamamoto K, Kanno T (2000) Endoscope-assisted microsurgery for cerebral aneurysms. Minim Invasive Neurosurg 43:91–97
King WA, Wackym PA (1999) Endoscope-assisted surgery for acoustic neuromas (vestibular schwannomas): early experience using the rigid Hopkins telescope. Neurosurgery 44:1095–1100; discussion 1100–1102
Perneczky A, Boecher-Schwarz HG (1998) Endoscope-assisted microsurgery for cerebral aneurysms. Neurol Med Chir (Tokyo) 38[Suppl]:33–34
Perneczky A, Fries G (1998) Endoscope-assisted brain surgery. I. Evolution, basic concept, and current technique. Neurosurgery 42:219–224; discussion 224–225
Perneczky A, Muller-Forell W, Van Lindert E (1998) Keyhole concept in neurosurgery with endoscope-assisted microsurgery. Thieme, Stuttgart
Takaishi Y, Yamashita H, Tamaki N (2002) Cadaveric and clinical study of endoscope-assisted microneurosurgery for cerebral aneurysms using angle-type rigid endoscope. Kobe J Med Sci 48:1–11R
Taneda M, Kato A, Yoshimine T, Hayakawa T (1995) Endoscopic-image display system mounted on the surgical microscope. Minim Invasive Neurosurg 38:85–86
Taniguchi M, Takimoto H, Yoshimine T, Shimada N, Miyao Y, Hirata M, Maruno M, Kato A, Kohmura E, Hayakawa T (1999) Application of a rigid endoscope to the microsurgical management of 54 cerebral aneurysms: results in 48 patients. J Neurosurg 91:231–237
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Profeta, G., De Falco, R., Ambrosio, G. et al. Endoscope-assisted microneurosurgery for anterior circulation aneurysms using the angle-type rigid endoscope over a 3-year period. Childs Nerv Syst 20, 811–815 (2004). https://doi.org/10.1007/s00381-004-0935-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-004-0935-1